St Mary`s Antimicrobial Stewardship
advertisement

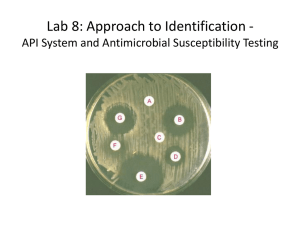
Antimicrobial Stewardship St. Mary’s Hospital Infection Control Committee What is Antimicrobial Stewardship • An interdisciplinary team dedicated to practices that improve appropriate selection, dosing, route, and duration of antimicrobial therapy • The ultimate goal of antimicrobial stewardship is to improve patient care and health care outcomes Antimicrobial Stewardship Team • • • • Infectious Disease Physician Clinical Pharmacist Clinical microbiologist Information System Specialist • Infection control professional • Hospital epidemiologist • Leadership support Elements of an Antimicrobial Stewardship Team • A comprehensive program will include: – Active monitoring of resistance – Fostering of appropriate antimicrobial use – Collaboration with an effective infection control program to minimize secondary spread of resistance is considered optimal Elements of an Antimicrobial Education Stewardship• Program • Prospective audit with intervention and feedback • Formulary restriction and preauthorization • Guidelines and clinical pathways • Antimicrobial cycling • Antimicrobial Order Forms • Monitoring of progress and outcome measures • De-escalation of therapy • Dose optimization • Conversion from parenteral to oral • Computer Surveillance/Decision Support • Microbiology Laboratory Prospective audit,intervention,and feedback • Have the clinical pharmacist on the floor making recommendations about appropriate antibiotic, route, length of therapy • Probiotic Protocol to prevent C. Diff • Focus on one floor for recommendations • Up to a 37% reduction in the number of days of inappropriate antibiotic use.Approx. $400.00 cost savings per patient • While assessing patients for probiotics look at deescalating of antibiotics • Decrease rate of C. Diff Formulary restriction and preauthorization • Restriction of requirements for specific agents • Control of certain antibiotic use through Pharmacy and Therapeutics Committee can be very effective • Control of Cleocin use has led to prompt cessation of nosocomial outbreak of C. Diff Vancomycin and third generation cephalosporins in response to VRE has demonstrated mixed results Education • • • • Conference Presentations Student teaching E-mail alerts Provision of written guidelines • Peri-operative area order forms • Share results of audits Guidelines and Clinical Pathways • Implementation of guidelines incorporating local microbiology and resistance patterns • Balance antibiotics in HAP and VAP patients • Use algorithms incorporating the clinical pulmonary infection score • Leads to decreased duration of therapy,decreased VAP recurrence, decrease of multidrug resistance patterns Antimicrobial Cycling • Slows spread of resistance • Most popular is Gentamicin to Amikacin • Ceftazadime for Ciprofloxacin lead to a decreased incidence of VAP Antimicrobial Order Forms • Use of Peri-operative prophylactic order forms with automatic stop at 2 days (SCIP Guidelines) • Pneumonia Order set (Pneumonia core measures) with 6 different pneumonia indications and drugs • Order forms facilitate implementation of practice guidelines Streamlining or De-Escalation of therapy • Continuing excessive broad therapy contributes to the selection of antimicrobial resistant pathogens • When culture results become available we can streamline or de-escalate antimicrobial therapy to more targeted therapy that decreases antimicrobial exposure and contains cost • This can also lead to avoidance of redundant inpatient antibiotic- days Dose Optimization • Dosing that accounts for individual patient characteristics (age,weight,renal function) • Site of infection • Pharmacokinetics Vancomycin and aminoglycosides • Optimize antimicrobial pharmacodynamics of the drugs B-lactams and fluoroquinolones Conversion from parenteral to oral therapy • Having a systematic plan for switching from parenteral to oral treatment may have an added benefit of aiding in early hospital discharge planning • Development of clinical criteria and guidelines allowing conversion can facilitate implementation. Computer Surveillance / Microbiology • Add cost codes to antimicrobial susceptibility data • Antimicrobial report to pharmacy • Vancomycin dosing/utilization sheet • Review antimicrobial errors • Leap frog to CPOE • Actively involved in resistance surveillance • Update antibiogram annually • Make easily accessible to physicians St.Mary’s Antibiotic Stewardship Efforts to Date • • • • • • • • Probiotic Protocol Antibiogram on line Pneumonia Order sets Pharmacokinetics Peri-op Area Guidelines IV to PO conversion Culture results from lab Pharmacy/IS generated pneumonia vaccine program What does our future hold for Antibiotic Stewardship • Assign antibiotic rounds to new pharmacy school professor ( de-escalating and streamlining) • Follow culture results from lab • Approve IV to PO conversion automatic by pharmacist • Finish 6 month Probiotic study • Work on Vancomycin Order form Antibiotic Stewardship 2013 140 18.5 120 18 100 17.5 80 60 17 40 16.5 20 0 -1 4 N ov p- 14 4 Se l-1 Ju 14 ay - 4 M ar -1 M Ja n- 14 16 #Interventions % Acceptance 15.5 1stQtr 2ndQtr 3rd Qtr 4th Qtr TARGET Athens cost per discharge Total Savings 2013 $15,458 Documentation of Interventions by type MONTH : SEPTEMBER 2013 Total Antibiotic Interventions:100 Percent Accepted: 85% Accepted Change Dose Change Antibiotic IV to PO conversion Discontinue Therapy Add an antibiotic Renal dosing Streamline 1 10 21 28 1 15 2 8 5 6 3 1 15 27 31 2 15 2 8 Not accepted Total 1 • April Ecker and Gin Fleming (Antibiotic Pharmacist) Other: Probiotic C.H.E. Act Initiatives Thru September 2013 Anti-infectives (Antibiotics) Anticoagulants 25 20 7 2011-2013 Target 6 5 15 Cost per adjusted discharge 10 5 0 Anticoag cost per adjusted discharge 3 2 1 3 l-1 13 Mar- Apr- M Jun- JulA Sep- Oct13 13 ay13 13 ug- 13 13 13 13 Ju 2 Ja n- 12 l-1 Ju Ja n- l-1 1 11 0 Ju Ja n- Target 4 Asthma Drugs 1 9 8 Proton Pump Inhibitors 0.95 7 0.9 6 Target 5 Asthma Drugs Cost per adjusted discharge 4 3 TARGET 0.85 PPI COST PER ADJUSTED DISCHARGE 0.8 2 0.75 1 0 12 N ov -1 2 Ja n13 M ar -1 3 M ay -1 3 Ju l-1 3 Se p13 Se p- -1 2 Ju l 12 M ay - M ar - 12 0.7 Mar13 Apr13 May- Jun13 13 Jul13 Aug- Sep13 13 Oct13 ACT-Medication Management Anti-Infective Stewardship Initiative 2010 $30.00 $25.00 2010 Target $20.00 $15.00 $10.00 $5.00 Ja nFe 1 0 bM 10 ar -1 A 0 pr M 10 ay -1 Ju 0 nJu 10 ly 20 A 1 ug Se 10 p1 O 0 ct N 10 ov -1 0 $0.00 Cost per adjusted discharge St. Mary's 2010 Target