Serial peak flows in the investigation of occupational asthma
advertisement

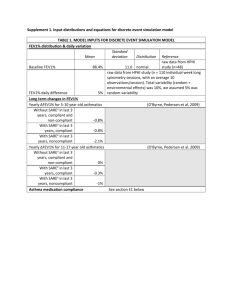
The management of work-related asthma OEMAC 2010 Jeremy Beach University of Alberta Potential conflicts of interest • Have received research funding from Alberta WCB and AHRQ. • Was a member of ACCP WRA guidelines committee • No shareholdings, payments or honoraria from pharmaceutical companies or equipment manufacturing companies. Learning objectives • Participants will understand the diagnosis and management of work related asthma based on the most recent guidelines • Participants will understand current issues surrounding surveillance of work related asthma including occupational asthma • Participants will understand elements of management including removal from exposure and the role of evidence based practice in the management of work related asthma Sources of information • • • • AHRQ systematic review ACCP guidelines BOHRF guidelines Cochrane review – specifically on workplace interventions • Other papers/guidelines/articles References at end Definition of work-related asthma • Occupational asthma- asthma caused or contributed to by an exposure at work: – With latency - sensitisers – Without latency – irritants, RADS • Work aggravated asthma – Pre-existing asthma made worse by simple physical exposure at work The Individual with work-related asthma Questions about management • Is complete removal from exposure necessary? – Is reduction of exposure adequate – Can PPE safely be used • Are there any specific medications of particular use in OA – Steroids after an acute exposure • What is the economic/social impact of OA for individual affected, and society AHRQ - Methods • Search terms identified • Indexing databases searched: – MEDLINE, EMBASE, Dissertation abstracts, Expanded academic, National Agricultural and Safety Database, CINHAL, Biological abstracts, Agricola, Trials registries, Web of Science, hand search, grey literature • Reviewed for relevance and quality • Relevant data extracted – Estimate sensitivity and specificity for diagnosis – Assess outcome for management Initial independent references from all databases (n=11366) Citations with potential relevance (n=632) First screening of titles and abstracts using general criteria 13 studies were assessed for diagnosis and management 16 studies were unobtainable Diagnosis Review Management Review Full text articles with potential relevance (n=493) Reference lists, authors’ lists, conference presentations * 33 studies waiting assessment Met inclusion criteria (n=109) Second screening with specific criteria Full text articles with potential relevance (n=152) Reference lists, authors’ lists, conference presentations Met inclusion criteria (n=58) Management • Needed to classify ongoing exposure status, while on optimal treatment – Continued unchanged – Reduced – Ceased Management • Most data available for FEV1, NSBPT, and use of medication for outcomes – see figures following – No metanalysis - heterogeneity • Symptoms – Removal – majority had some improvement • Few had complete resolution – Exposed – continued unchanged or deteriorated 20 Removed 10 Exposure v FEV1 0 Change in Average %predicted FEV-1 -10 -20 0 2 20 4 6 8 6 8 Exposed 10 0 -10 -20 0 2 20 4 Reduced 10 0 W - HMW -10 B - LMW -20 0 2 4 6 8 Length of Follow-up (years) Size of plotting character is proportional to number of patients follow ed G - mixed 4 Ratio of Follow-up and Baseline Mean Hyperesponsiveness Exposure v NSBPT Removed 5 3 2 1 0 0 2 4 6 8 6 8 Exposed 5 4 3 2 1 0 0 2 4 Reduced 5 4 3 W - HMW 2 1 B - LMW 0 0 2 4 6 8 Length of Follow-up (years) Size of plotting character is proportional to number of patients follow ed G - mixed Removed 100 Exposure v medication use 80 60 40 20 Percent of Patients on Medications 0 0 2 4 6 8 10 12 14 10 12 14 Exposed 100 80 60 40 20 0 0 2 4 6 8 Reduced 100 80 60 W - HMW 40 20 B - LMW 0 0 2 4 6 8 10 12 14 Length of Follow-up (years) Size of plotting character is proportional to number of patients follow ed G - mixed Cochrane Review: WORKPLACE INTERVENTIONS FOR TREATMENT OF OCCUPATIONAL ASTHMA • INTERVENTIONS : • 12 Stop Exp v Continue Exp • 3 Less Exp v Cont Exp • 2 Stop Exp v Less Exp • 1 Education • Total: 15 English articles • - AGENTS : 4 Western Red Cedar 3 TDI 2 NRL 2 Various 1 Cobalt 1 Colophony 1 Potroom 1 Mixed farming Cochrane review – pre pelininary Risk Ratio, M-H, Random, 95%CI Systematic review - Rachiotis • Patients with shortest duration of exposure had highest rate of recovery But • Effect not linear • No clear patterns in between-study comparisons Results - Trials • Two studies suggest inhaled steroids (5-6 months) help recovery once exposure ceases. • Little other good evidence. Effectiveness of medication probably similar to non WRA. Results - Trials – Wheat flour immunotherapy: • Decreased serum specific IgE; • Less skin prick sensitivity; • Less non-specific bronchial reactivity. – Fel d1 effective in non-OA – Respiratory PPE significantly improved specific airway resistance. – Use of low protein hypoallergenic gloves reduced asthma exacerbations. Citation Removed/Unemployed Exposed or Reduced -84 percent (69/82^) -$4,203.72 USD/year -$5,863.88 USD/year -54 percent (56/78^) 39/112 unemployed -$368.14 USD/month -$609.96 USD/month* 53/128 unemployed -19 percent (20/104^) -$268.71 USD/year -$3820.27 USD/year -35 percent (14/34^) -$12.46 USD +$13.17 USD Income Ameille et al. Moscato et al. Gannon et al. Marabini et al. Pharmaceutical Costs/month Moscato et al. -$256.38 USD/month Note: * = unemployed; + = reduced exposure; ^ = perception of reduced income Financial consequences • OA results in loss of income • Greatest loss was in those removed from workplace, but even those who stayed with same employer lost income. • Drug costs higher in those with ongoing exposure • Unemployment a relatively common outcome Compensation • In Canada WCB system – Recognition and reporting a prerequisite – Often straightforward with clear case of sensitiser induced OA – Can be much more difficult when information on exposures is difficult to obtain, or when disease difficult to characterise – irritant OA v WEA v COPD Management of work-related asthma at a business/societal level • Questions – Is primary prevention effective? – Is health surveillance useful in a workplace with asthmagen exposure – How can long term consequences/costs be minimised. Primary prevention • Risk assessment • Hierarchy of control – Some evidence of success • Substitution – latex gloves • Encapsulation of detergent enzymes – control • Autobody painters, acid anhydride manufacture – PPE • Recognising case as sentinel event Heath surveillance • Pre-employment – Atopy/smoking are risk factors. • Common characteristics - discrimination • No evidence excluding significantly reduces risk • Periodic – Sensitisation • Probability of progression high once sensitised – Disease • Difficulty of finding sensitive and specific test • Importance of education/awareness • Estimated cost per case of disability prevented = US $64,000 Minimising costs and consequences • Estimated mean compensation cost of a case of OA in Quebec 1998-2002 >$90,000 • Factors associated with increased cost • • • • Male Age >40 LMW agent Severity of disease (FEV1 <80%/use of inhaled steroids/PC20 <16 mg/ml) • Changing employer • >1 year with symptoms prior to diagnosis Factors associated with increased time to diagnosis • Age > 40 • Salary >$30,000 - possibly • OA due to HMW ? Worth focussing surveillance Conclusions - management • Those with OA who remain exposed tend to experience decreased FEV1, increased NSBR, and will usually require medication. • Those with OA who cease exposure tend to experience improved FEV1 and decreased NSBR. The majority still require ongoing medication use. • The majority of those who cease exposure report ongoing symptoms, and some experience decreasing FEV1 despite exposure ceasing Thank you Questions References/reading 1. 2. 3. 4. 5. 6. 7. 8. Beach J, Rowe BH, Blitz S, Crumley E, Hooton N, Russell K, Spooner C, Klassen T. Evidence Report/Technology assessment No. 129. Diagnosis and management of work-related asthma. AHRQ Publication No. 06-E003-2. Rockville MD: Agency for Healthcare Research and Quality, 2005. Tarlo SM, Balmes J, Balkissoon R, Beach J, Beckett W, Bernstein D, Blanc PD, Brooks SM, Cowl CT, Daroowalla F, Harber P, Lemiere C, Liss GM, Pacheco KA, Redlich CA, Rowe B, Heitzer J. ACCP Consensus Statement: Diagnosis and Management of Work-related Asthma. Chest 2008; 134 (3 Suppl): 1s-41s Newman Taylor AJ, Nicholson PJ, Cullinan P, Boyle C, Burge PS. Guidelines for the prevention, identification& management of occupational asthma: evidence review and recommendations. BOHRF, London, 2004. Rachiotis G, Savani R, Brant A, MacNeill SJ, Newman Taylor A, Cullinan P. Outcome of occupational asthma after cessation of exposure: a systematic review. Thorax. 2007; 62: 147-52. Malo JL, L’Archeveque J, Ghezzo H. Direct costs of occupational asthma in Quebec between 1988 and 2002. Can Respir J 2008; 15: 413-416. Miedinger D, Malo JL, Ghezzo H, L’Archeveque J, Zunzunegui M-V. Factors influencing duration of exposure with symptoms and costs of occupational asthma. Eur Repir J 2010, published on line de Groene G, Pal TM, Verbeek JH, Beach J, Tarlo SM, Frings-Dresen MHW. Workplace interventions for treatment of occupational asthma. Cochrane Database of Systematic Reviews 2007 , Issue 1 . Art. No.: CD006308. DOI: 10.1002/14651858.CD006308 Wild DM, Redlich CA, Paltiel AD. Surveillance for isocyanate asthma: a model based cost effectiveness analysis Occup Environ Med 2005; 62: 743-749. Cochrane review Pre-Pre-liminary results: Improvement of Asthma Symptoms