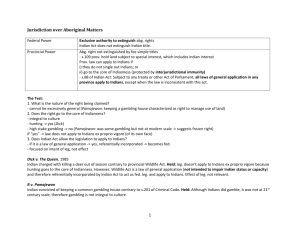
Endotracheal Suctioning: Benign Procedure or Please Use Caution?
advertisement

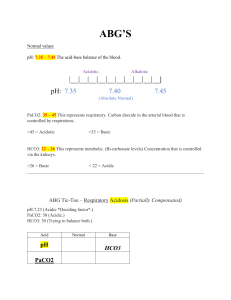
Interactive Case Studies In Respiratory Care Doug Pursley, M.Ed., RRT Program Director Ozarks Technical Community College Springfield, MO Case 1 • A 74 year old female with COPD is admitted to the ED with mild chest pain. She is on her portable liquid system at 3 l/m. • B/S, CXR clear, pt. is alert and oriented • ABGs: pH 7.32, PaCO2 84, HCO2 42, BE +15, PaO2 68 • The physician sees the initial ABG and wants to place the patient on BiPAP. • The RCP disagreed and convinced the physician that BiPAP is not indicated at this time since the patient is not in respiratory distress and has “classic” chronic hypercarbia. • She is moved to a regular room from triage to await labs and speak with the physician • 30 minutes later the physician pops his head in the door and finds the patient lethargic and on 10 l/m per nasal cannula. • ABG at this time is: pH 7.20, PaCO2 110, HCO3 41, BE +13, PaO2 117 • Now she is BiPAPed 10/5 and 40% • Next ABG shows: 7.22, PaCO2 103, HCO3 41, BE +13, PaO2 64 • The patient’s BiPAP settings are changed to 15/5 and she is transferred to the MICU. • She is removed from BiPAP a few hours later and had the following ABG on 3 l/m: pH 7.30, PaCO2 87, HCO3 41, BE +14, PaO2 61 • Obviously a case of oxygen-induced hypercarbia Case 2 • A 53 year old female with diabetes and COPD is admitted to the ED. • She walks in under her own power and has the following ABG drawn 10 minutes later: pH 6.65, PaCO2 76, HCO3 8, BD -25 • Glucose 620, increased WBCs • She is placed on BiPAP 20/15, 100% for a few minutes and then intubated • She develops asystole as she is being intubated and is resuscitated unsuccessfully for 45 minutes. Case 3 • The patient is a 34 year old male that has just been brought to the ETC after a narcotic overdose. He is currently being mechanically ventilated. What is your recommendation after seeing his CXR? Case 4 • 450 lb. 45 year male is brought to a local ETC (PB 730 mmHg) in acute respiratory distress. Someone places him on a nasal cannula but they forget to turn the O2 on. He is also placed on a pulse oximeter and ABG’s are drawn. • Good pleth waveforms are seen on the pulse oximeter which measured 81% at the time the ABG was drawn. Ten minutes later, you arrive, turn the oxygen on, and titrate the O2 achieving an SpO2 of 94%. • The patient’s vital signs improve and he says he is less short of breath. ABGs on room air were: FI02 pH PaC02 HCO3 Base Pa02 Sp02 .21 7.33 64 32.6 +7 84 81% (at time of blood draw) What is your recommendation after seeing the ABG? Case 5 • K.B. is a 55 kg., 72 year old documented CO2 retainer with end-stage COPD who also has a history of severe air trapping and dynamic flow limitation. • Admitted the previous day for exacerbation of his COPD. • Intubated and placed on a ventilator after failing NIV. • Current ventilator settings are: PRVC, 500 X 16 (total f 16), Set PEEP 5, and FIO2 0.35 • Total PEEP is measured at 10 cmH2O • • • • • • • • ABG’s on those settings are: pH 7.50 PaCO2 40 mmHg HCO3 30.1 BE +6 PaO2 65 SaO2 94% Hb 18 g% What is your recommendation? Case 6 • An 8 year old boy is brought to the ETC after being hit by a car while walking across a Walmart parking lot. • He was intubated prior to arrival and is currently being manually ventilated. • A chest x-ray is taken with the boy in the supine position. The CXR shows an ETT just inside the RMS and fractures of the 4th and 5th posterior ribs on the right. What other major finding is seen on the CXR? What is the major finding? 1. 2. 3. 4. Left pleural effusion Right pneumothorax Left pneumonia Pulmonary edema His ABG’s are: pH 7.19, PaCO2 60, HCO3 22. Interpretation? Case 7 • You are taking care of a post-op cholecystectomy patient on a 40% ventimask. The recommended flow stamped on the device is 6 l/m, which is what the device is set for. • On further examination, you notice that the patient’s work of breathing seems to be slightly increased and that her SpO2 is 88% • You then perform a quick calculation and determine that the total flow exiting a 40% ventimask running @ 6 l/m is 24 l/m (3:1 ratio) and remember your old instructor in school saying that a normal, resting inspiratory flowrate for an adult is about 25-35 l/m. • What is the most appropriate action to take at this time? Most appropriate action? 1. Take her off the venti and place her on a 6 l/m cannula 2. Increase the FIO2 on the ventimask to 50% 3. Increase the flow on the 40% ventimask 4. Do nothing. The stamped flow says 6 therefore it has to be set on 6. Case 8 • A nurse hears cries of help from a 64 year old female COPD, lung cancer patient. She is on oxygen. • When she gets to the patient’s room, she finds the O2 tubing, pillow, and patient’s hair on fire. • She quickly extinguishes the fire but the patient suffered burns to the face, neck, right shoulder, and upper back while trying to light a cigarette. • The patient is then transferred to the Burn Unit. • According to data from the Consumer Product Safety Commission, approximately how many medical oxygen related thermal burns were seen in US emergency rooms in the four years from Jan 1,2003 to Dec 31, 2006? FIRES AND BURNS INVOLVING HOME MEDICAL OXYGEN Marty Ahrens Fire Analysis and Research Division National Fire Protection Association August 2008 How many O2 induced thermal burns do you think were reported in the US from Jan 1, 2003-Dec 31, 2006? 1. 2. 3. 4. 1,000 5,000 25,000 100,000 Case 9 • A 76 year-old, 58 kg IBW, male is admitted with extreme hypothermia Vitals on admission • • • • • Temperature 30 C Pulse 74 f 41 and shallow Crackles Atrial fibrillation 76 year-old, 58 kg IBW • In the ER he is placed on a ventilator with the following settings: PC, pressure 23 cmH20, f 12, PEEP 8, FIO2 0.35, exhaled tidal volume 570 ml. • ABG’s reported at 37 C are: • pH 7.40 • PaCO2 40 • PaO2 80 • Because he was hypothermic when the blood gas was drawn, the physician requested that the lab correct the ABG to 30 C. • The corrected ABG is: • pH 7.50 • PaCO2 30 • PaO2 54 • The ER doc asks for your opinion on what ventilator changes to make. • What is your recommendation at this time? What is your recommendation? 1. Decrease rate from 12 to 8 2. Increase FIO2 from 0.35 to 0.60 3. Increase PEEP from 8 to 15 4. Do all three 5. Make no changes at this time 37 C 30 C pH PaCO2 PaO2 7.40 40 80 7.50 30 54 Case 10 • A 64 year old male presents to the ED with extreme shortness of breath. A CXR is obtained. What immediate treatment is indicated? 1. 2. 3. 4. 5. IPV Bilalateral chest tubes Bronchoscopy Albuterol and CPT Q2 CPAP and 40 mg of Lasix Case 11 • A 37 year old male presents with bronchial breath sounds and crackles in the left lower lobe, E to A egophony on the left, increased tactile fremitus on the left, dull percussion note on the left, and decreased chest expansion on the left. What do the findings suggest? 1. 2. 3. 4. 5. Pneumothorax Pneumonia Pleural effusion Bronchitis Asthma Case 12 • A 40 kg., 32 year old female MVA is being ventilated and has a 6.0 ETT in place. • She is currently being suctioned with a 14 F catheter. • You and a co-worker get into a discussion about the proper size of catheter to use on a 6.0 ETT What is the ideal suction catheter size for a 6.0 ETT? • • • • 1. 10 F 2. 12 F 3. 14 F 4. Doesn’t matter Case 13 • Just as you are about to go home for the day, you notice a group of people in the ED gathered around the lateral neck x-ray of a 13 year old male just admitted for extreme shortness of breath. The lateral neck x-ray shows: 1. Epiglottitis 2. Croup 3. Foreign body obstruction 4. Retropharyngeal abscess 5. Cervical fracture