oncologic emergencies
advertisement

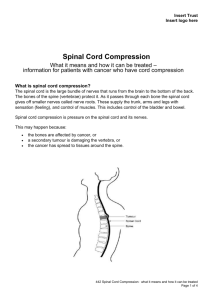
Oncologic Emergencies Dr Karenza Alexis Spinal Cord Compression 1-5% of patients with systemic cancer MUST BE TREATED IMMEDIATELY Can lead to irreversible paralysis or loss of bowel and bladder function Tumor or collapsed fragments in the epidural space Spinal Cord Compression Most Common sites Thoracic spine (70%) Lumbrosacral (20%) Cervical (10%) Most common malignancies Lung Breast Unknown primary Prostate Renal Multiple myeloma Lymphoma Spinal Cord Compression Symptoms and Signs Localized pain to the spine Exacerbated by movement, recumbency, coughing, sneezing, straining May appear weeks to months before neurological symptoms Radicular pain Weakness +/- sensory loss Autonomic dysfunction Urinary retention, constipation Spinal Cord Compression Evaluation- complete neurologic and physical exam that includes: Gentle percussion of spinal column Passive neck flexion Straight Leg raise Motor and sensory exam, Reflexes Pinprick testing toe to head- sensory level Is there a “sensory level” RECTAL exam Spinal Cord Compression Diagnosis- image the ENTIRE spine Xray MRI 66% will have bony abnormalities Erosion, loss of pedicles, vertebral body collapse, paraspinous soft tissue mass Cannot exclude epidural mets Does not exclude cord compression if normal Follow-up with MRI STANDARD!!!!!!! CT scan Spinal Cord Compression Goal of treatment: recovery and maintenance of normal neurological function, stabilization of the spine Local tumor control pain control Treatment Outcome: Degree of neurologic impairment Radiosensitivity of tumor Spinal Cord Compression Treatment: Steroids START DEXAMETHASONE IMMEDIATELY if you suspect cord compression 10 mg IVP followed by 4 mg IV every 6 hours (higher doses be used if patient presents with significant neurological impairment) Radiation Stable spine with radiosensitive tumors, nonsurgical candidates with spinal instability, Port includes area of epidural involvement plus two vertebral bodies above and below Spinal Cord Compression Surgery Tissue diagnosis needed Spinal instability Prior radiation to affected area Progression of cord compression despite steroids and radiation Resection followed by radiation therapy vs radiation alone ASCO proceedings 2003: combine modality patients had higher ambulatory rate and retained ability to walk longer Spinal Cord Compression In addition to initial evalutaion, imaging, steorids: multidisciplinary management Neurology Consult Oncology Consult Neurosurgery Consult Radiation oncology Consult Superior Vena Cava Syndrome Malignant causes intrathoracic malignancies (60-85%) Lung cancer (more common in small cell), breast cancer, testicular cancer, thymoma lymphoma and other malignancies with mets to mediastinum Non-malignant causes Thrombosis (most common cause in cancer patients) Substernal thyroid goiter, TB, RT, sarcoidosis Superior Vena Cava Syndrome Signs and symptoms Facial edema/ erythema Dilatation of veins of upper body Laryngeal or glossal edema Periorbital edema Dyspnea Cough Orthopnea Arm and neck edema Hoarseness Dysphagia Headaches Dizziness syncope Symptoms worse with positional changes: bending forward, stooping or lying down Superior Vena Cava Syndrome Can Result in: Life-threatening Laryngeal cerebral edema edema- airway compromise Superior Vena Cava Syndrome Diagnosis- determine etiology Thorough Physical Examination CXR May show mediastinal widening Doppler USG of jugular or subclavian vein Differentiate thrombus from extrinsic compression CT scan or MRI Bronchoscopy thoracoscopy Superior Vena Cava Syndrome Treatment Goal: alleviate symptoms and treat underlying disease Initial management depends on Grade of SVCS, underlying disease, anticipated resposbse Determine underlying cause- especially if SVCS is presenting symptom Pace of progression of symptoms Treatment goal- Cure vs Palliation Superior Vena Cava Syndrome Treatment Symptom management: Elevation of head of bed, O2, bed rest Radiotherapy Cure vs Palliation Accurate histologic diagnosis needed prior EMERGENT RT needed if life-threatening symptoms/signs (stridor/ CNS symptoms from cerebral edema) If Non-small cell lung cancer Combine with chemotherapy if limited stage small cell lung cancer and NonHodgkin’s lymphoma Stenting for life threatening symptoms especially in tumors not sensitive to chemotherapy or radiation or no diagnosis of cancer Chemotherapy Lymphoma or germ cell tumor or small cell lung cancer Consider thrombolysis, angioplasty if thrombosis Diuretics- transient, may cause dehydration and reduced blood flow Steroids Hypercalcemia Occurs in 10-20% of cancer patients- bony mets v paraneoplastic Assocciated most commonly with: myeloma, lung cancer (squamous cell), renal cancer, breast cancer, head and neck tumors, leukemias, unknown primaries Hypercalcemia Symptoms/ signs Presence may depend on speed at which hypercalcemia develops General: dehydration, anorexia, pruritis, weight loss, fatigue CNS: weakness, hypotonia, proximal myopathy, mental status changes, seizure, coma Cardiac: bradycardia, short QT interval, prolonged PR interval, wide T wave, atrial or ventricular arrythmias GI: nausea/vomiting, constipation, ileus, pancreatitis, dyspepsia Renal: Polyuria, nephrocalcinosis Hypercalcemia of malignancy Diagnosis Ionized calcium, Serum immunoreactive PTH- like substance, phosphorus, 1,25 dihydroxyvitamin D If calcium only mildly elevated (<12) AND NO symptoms: encourage PO hydration, eliminate any offending agents, follow closely If calcium is >12 OR symptoms: saline infusion (be aware of cardiac and renal function), loop diuretics (once euvolemia achieved). Follow urine output and potassium, magnesium. Bisphosphonates inhibit osteoclast function e.g pamidronate Onset of action 24 to 48 hours Calcitonin Inhibits bone degradation by binding directly to receptors on the osteoclast onset of action is 2-4h but effect of short duration. Dose is 2-8 U/kg SC or IM every 6-12 h If calcium >12 or symptoms Gallium nitrate- inhibits bone resorption Onset of action 24 to 48 hours 100-200 mg/m2/d IV over 24 hours for up to 5 days in volume replete non-oliguric patients Once calcium is normal, stop treatment but CONTINUE TO MONITOR for its continued effect AVOID use of nephrotoxic drugs Plicamycin (25 ug/kg) Direct osteoclast inhibitory effects, may also block Vit D and PTH activity Onset of action is 24-48 h Toxicity with repeated use: renal and liver toxicity, thrombocytopenia Tumor Lysis Syndrome Metabolic triad of hyperuriciemia, hyperkalemia, hyperphosphatemia Can also lead to renal failure and hypocalcemia as secondary complications Chemotherapeutic agents cause cell lysis and cell death with release of intracellular components into the blood stream Breakdown of nucleic acid, catabolism of hypoxanthine and xanthine leads to elevated uric acid Potassium and phosphate are present at high levels in cytoplasm LDH also released but not considered part of syndrome Tumor Lysis Syndrome Risk Factors, Signs or Symptoms Increased LDH, uric acid, creatinine Bulky, rapidly proliferating tumors treated with chemotherapy Most often occurs with treatment of leukemias or high grade lymphomas Cardiac arrythmias if hyperkalemia or hypocalcemia Tetany if hypocalcemia Renal failure if hyperphosphatemia and hyperuricemia Tumor Lysis Syndrome Prophylaxis Patient at high risk: leukemia, high grade lymphma, rapidly proliferating bulky solid tumor (e.g small cell) Vigorous Prehydration Allopurinol Inhibits xanthine oxidase Can cause xanthinuria Prevents new uric acid formation Careful Metabolic monitoring Treatment Rasburicase (works for prevention and treatment) degrades uric acid to more water soluble form Contraindicated in G6PD deficiency Can cause hemolysis Hyperuricemia Hematological disorders: leukemias, high-grade lymphomas, myeloproliferative disorders (e.g PCV) Aggressive tumors, extensive disease Treatment of malignancies Medications Renal impairment Hyperuricemia- treatment Prophylaxis Alkalinization of urine (urine pH >7) Sodium bicarbonate to IVF Diamox Allopurinol Neutropenic Fever Medical Emergency Neutropenia: ANC<1000 (multiply total wbc by percentage neutrophils and bands) Single temperature greater than 101.3F or sustained temperature >100.4F for more than one hour (for clnical purposes , single temo>100.4F) Remember there may still be infection in the absence of fever: e.g elderly patients or patients on steroids May present with hypothermia, hypotension, clinical deterioration START BROAD SPECTRUM ANTIBIOTICS ASAP!!!! Neutropenic Fever Risk factors for occult infection Degree of neutropenia Rapid decline in ANC Prolonged duration neutropenia (> 7 to 10 days) Cancer not in remission Comorbid illness Peripheral lines and central venous catheters Use of monoclonal antibodies Neutropenic Fever Infectious source identified in 30% 80% infection believed to arise from patient’s endogenous flora Risk for specific types of infection may be influenced by underlying malignancy Abnormal antibody production in CLL, functional asplenia: encapsulated organisms- Strep pneum.,hemophilus influenzae, Neisseria meningitidus, capnocytophaga canimorsus T cell defects e.g lymphoma: intracelluar pathogensListeria monocytogenes, Salmonella, Mycobacterium, Cryptococcus High dose steroids: Pneumocystis carinii ALWAYS COVER Gram negatives Fungal and viral infections also possible Neutropenic Fever Patients should be pancultured including from central line as well as CXR Further imaging depending on symptoms Generally start cefipime 2g Q8 (also take into consideration signs, symptoms, recent antibiotic use) GROWTH FACTOR support Consider vancomycin if hypotension,mucositis, skin infection, presence of catheter, hx MRSA, recent quinolone Addition of antibiotics (including antifungal) depending on clinical response and duration of neutropenia (add antifungal if anticipate or patient has prolonged neutropenia) Consider catheter removal Oncology Consultation Infectious disease consultation