Case presentation - Mymensingh Medical College
advertisement

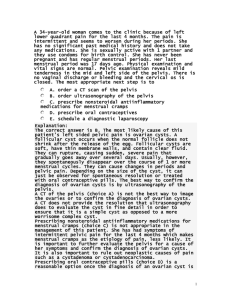
A 35 years lady presented with 12 weeks amenorrhoea with per vaginal bleeding. Dr. Atia Afreen DGO Student Mymensingh Medical College Particulars of the Patient Name: Mrs. Yasmin Age: 35 years Religion: Islam Occupation: House Wife Address: Bank Colony, Jamalpur. Date of admission: 12th March 2012 Date of examination: 12th March 2012 Pregnancy for 12 weeks. Per vaginal bleeding for one day Mild lower abdominal pain for 12 hours. History of present illness According to the patient’s statement, she was reasonably allright 12 weeks back. Then she became pregnant with the usual sign symptoms of pregnancy. She had no h/o antenatal check up. About one day prior to her admission she noticed sudden onset of per vaginal bleeding. At first bleeding was scanty in amount which was increasing gradually & was aggravated by minor stress like defaecation & diminished by rest. History of present illness……. She also complained of mild lower abdominal pain which was intermittent and radiating towards the back. Pain was not associated with nausea & vomiting. Her bowel & bladder habit was normal. With the above mentioned complaints she was admitted in this hospital for proper management. History of past illness She had no history of D.M., HTN, Tuberculosis, & other medical diseases. She had undergone LUCS for three times. The last LUCS was performed on February,2008. Personal History: Nothing contributory Family History: Nothing contributory Socio-economic History: Belongs to middle class family. Immunization History: She is immunized against Tetanus & Hepatitis B virus as per schedule. Drug History: Nothing contributory. Contraceptive History: Couple practiced barrier method . Menstrual History • • • • • • Menarche: at the age of 13 years Menstrual period: 3-5 days Menstrual cycle:28±2 days Menstrual flow: averege LMP:10/12/2011 EDD: 17/09/2012 Obstetrical History Married for Gravida Para Stillbirth ALC : : : : : 16 years 4th 3(LUCS)+0 1 4 years General Physical Examination Appearance: Anxious Body built: Average Dicubitus: On choice Weight: 60 kg Height:5 ft 3 inches Pulse: 90 beats/min Blood pressure: 100/70 mm of Hg Respiratory rate:18/min General Physical Examination…. Temperature: 36.5⁰ c Anaemia/ Pallor:mild Jaundice: absent Cyanosis:absent Oedema:absent Dehydration-nil Lymphnode: not palpable Thyroid gland: not enlarged Systemic Examination Cardiovascular system Respiratory system Alimentary system Nervous System : : : : NAD NAD NAD NAD PER ABDOMINAL EXAMINATION Inspection: Umbilicus was centrally placed & inverted. A transverse scar measuring about 4” was present 1” above the symphysis pubis. Palpation: Abdomen was soft and non tender. Fundal height-not palpable Percussion: not done. Auscultation: Bowel sound present Pelvic Examination o o o Inspection: Vulva and vagina :Looks apparently healthy. P/V bleeding-present Per Speculum Examination: Cervix was broad,bluish in colour. Fresh blood comes out from os. Bimanual Examination: Cervix was soft, broad,distended & the uterus was about 12 weeks of size.OS was closed. Fornices were not tender & had no adenexal masses. SALIENT FEATURES Mrs. Yasmin 35 years old, housewife , 4th gravida with h/o three LUCS at term was admitted on 12th March 2012 at her 12 weeks of pregnancy with the complaint of per vaginal bleeding for the past one day associated with mild lower abdominal pain which was intermittent in nature. She seeks medical advice as per vaginal bleeding was gradually increasing. SALIENT FEATURES….. Her medical history was unremarkable, with no previous h/o pelvic inflammatory disease, or insertion of intrauterine devices. She practiced barrier method for contraception. Her menstrual cycle was regular with average flow. On examination the patient was found anxious, mildly anaemic, non icteric & non oedematous. Her blood pressure was 100/70 mm of Hg, pulse-90 beats/min. SALIENT FEATURES….. The abdomen was soft & no evidence of tenderness, guarding and rigidity. Pelvic examination revealed vulva &vagina apparently healthy, Cervix was soft, broad & distended & the size of uterus was about 12 weeks . Os was closed with fresh bleeding escaping through os. No fornicial tenderness & had no adnexal masses. Clinical Diagnosis 4th gravida with threatened abortion with previous h/o three c/s DIFFERENTIAL DIAGNOSIS Cervical ectopic pregnancy Pregnancy with cervical fibroid Molar pregnancy. Investigations General Blood for Hb: 9.8 gm/dl Random blood sugar: 5.7 mmol/L Blood grouping & Rh typing: B positive VDRL Test: Non reactive Urine R/M/E: Sugar-nil Pus cell-1-2/HPF Albumin-nil RBC-nil Investigations…… Specific Ultrasonogram of lower abdomen-12+1 weeks of gestational age of cervical pregnancy with empty uterine cavity. Serum beta HCG- 20,000 IU/L Confirmed diagnosis 4th gravida with 12 weeks cervical ectopic pregnancy with previous h/o three c/s. Management AIM- Termination of pregnancy Management… Definitive managementTermination of pregnancy was done by dilatation,evacuation & currettage under general anaesthesia. Curettage revealed products of conception from the distended cervical canal. The amount of product curetted out corresponded to about 12 weeks of pregnancy. Management……… Profuse haemorrhage continued despite of curettage and pressure, the cervix appeared like a elongated flabby loose fold of tissue. Foley’s catheter tamponade was attempted, failing which exploratory laparotomy with total abdominal hysterectomy was performed to save the life of patient. Patient was taransfused 3 units of blood peroperatively. Management……… After hysterectomy specimen was sent for histopathological examination. Management……… Her post operative period was uneventful and she recovered well.