The Keys to a Successful Audit
Appeals Program
Larry Hegland, MD, MMM
System Medical Director for Recovery Audit and Appeal Services
Chief Medical Officer: Ministry Saint Clare’s Hospital, Ministry Good
Samaritan Health Center and The Diagnostic and Treatment Center
Insert large graphics
on this slide.
RAC Structure
• Centralized RAC team serving Ministry
Health Care System with dedicated staff
–
–
–
–
–
Medical director (0.5)
Administrative director (0.5)
Audit and appeal nurses (4)
Database coordinators (4)
Local site liaisons
• Administrative
• Health information management
• RAC Steering Committee
• RAC tracking software
• Document management system
Ministry RAC Summary
•
•
•
•
Greater than $50 Million at risk
5156 complex reviews
>600,000 pages of documentation submitted
80% no findings rate
– 15.5% overpayment
– 4.5% underpayment
• Appeal rate: 75%
– 86% of closed appeals have been won
• What about the money?
– $0 Recouped for failure to meet a deadline or
properly follow the rules
– Recoupment <3% overall of at risk dollars
– Underpayments and appeals >3% overall
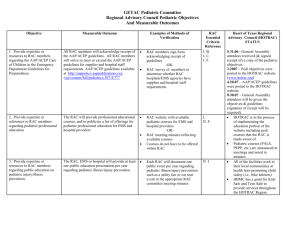
Rationale For Our Structure
Federal Auditors
2
US Department of
Health & Human Services
CMS
OIG
Centers for Medicare
& Medicaid Services
Medicaid
Office of Inspector General
Medicare
ZPIC
Zone Program Integrity
Contractors
MIC
Medicaid Integrity Contractors
RAC
Recovery Audit Contractors
(Post-payment, Automated & Complex)
PERM
Payment Error Rate Measurement
MAC
Medicare Administrative Contractor
Prepayment Probes
From the FI
(Fiscal Intermediaries)
CHIP
Children’s Health Insurance Program
RAC
Recovery Audit Contractors
CERT
Comprehensive Error Rate
Testing
RAC
Recovery Audit Contractors
(Pre-payment & Semi - Automated)
Constantly Shifting RAC Landscape
• 2012
–
–
–
–
Increased record request limits
Part A/B and RAC Prepayment demonstration projects
Everyone wants in on the RAC-style action
Administrative Law Judges and Part B
• 2013
– New CMS Ruling and Proposed Regulation for Part B
rebilling
• Self denial of Part A with Part B rebilling
• New billing rules
–
–
–
–
New record request limits and audit rules
Medicaid RAC
Unofficial 2013 Statement of Work changes
Predictive analytics/OIG validation audits
Keys to Success
It Starts With Dedicated Resources
• Optimum results require staff who:
– are trained to respond to recovery audits
– have time to keep up with the constant flow of program
changes
– can keep track of the little details to ensure that auditor and
fiscal intermediary errors are caught
– can do follow-up education to help prevent future billing
errors
• Poor results achieved when staff must squeeze audit
response work into an already over burdened
workload without training or ongoing education
• For systems, a critical piece of the dedicated
resources approach is to centralize RAC operations
– Experience helps drive improved performance
Advantages of Centralization
• Improved consistency, coordination and quality of
RAC efforts across system
• Allows for a more professional staff using processes
that are easier to manage
• More efficient communication with RAC auditor and
fiscal intermediary (including an audit trail) as well
as internal stakeholders and external consultants
– Focus on respectful relations with no demonizing of the
RAC program
• More efficient and effective management of appeals
process
• Can react more quickly to new audit types, rule
changes, auditor “errors” and other problems
Advantages of Centralization
• Improved capabilities to monitor auditor activities
• Allows for more extensive report production
• Easier to capture opportunities for improvement and
helps drive system process improvement efforts to
reduce future audit risk
– Coding
– Development of a physician advisor program
– Standardization of case management use of criteria
• Improved justification of technology use and costs
(RAC tracking software and document management
system)
• Reduced overall administrative cost to system (?)
Focus on Process
• Hire right
– Talent and professional diversity – nurses,
coders, administrative backgrounds
– Skill diversity – writing, database management
• Dedicated physician support/leadership
– Appeals, ALJs, education, management
– Can tie coding, documentation improvement,
case management and utilization review together
• Positive, high performance culture
– A team effort including internal experts
– No negative energy/do not demonize RAC
Focus on Process
• We are extremely methodical with a process in
place for every aspect of the audit process from first
receipt to when we finally close an account
– Meticulous account tracking with our RAC tracking software
– We prepare a case summary for each denial
• Includes RAC argument, key components of the patients chart
(from document management system), the opinion of the
nurse reviewing the case and any others involved in the
review, relevant source material such as Coding Clinics and
clinical literature
• Developed as part of the decision process to appeal and
updated as the appeal progresses
– All appeal letters prepared as if going to the Administrative
Law Judge and include clinical and legal arguments
Opportunity for Value Creation
• Direct feedback to coders and providers
• Documentation improvement education
– Excisional debridement, sepsis and etc.
•
•
•
•
Coding newsletter related to RAC issues
RAC Relief listserv
Order set development for CPOE system
Meetings with case management, health
information management and compliance
• Education for boards, management teams
and medical staff
– Intranet site with dashboard
– Detailed audit summaries provided
A Bigger Role for Physicians
• Physician support role (physician advisors)
–
–
–
–
–
Clinical knowledge and “complex medical judgment”
Understanding how documentation translates into coding
Can develop a high level of experience managing appeals
Reduce the need to involve individual physicians/timeliness
More reliable support to the ALJ hearing process
• Physician leadership role
– Can more effectively turn audit lessons into physician and
staff education
– Integrate coding, documentation improvement, case
management and CPOE
– Turn audit lessons into clinical/documentation process
improvement to improve patient care and prevent future
audit denials
Questions?
• For additional information or to be
added to the RAC Relief Listserv,
please direct requests to:
larry.hegland@ministryhealth.org
or
http://groups.google.com/group/rac-relief
or
715-393-2487
 0
0