Cardiovascular Disease in
Women: the Yentl Syndrome
Gender-related Issues in Medicine
UCLA December 11, 2012
C. Noel Bairey Merz, M.D., F.A.C.C, F.A.H.A
Women’s Guild Endowed Chair in Women’s Health
Barbra Streisand Women’s Heart Center
Preventive and Rehabilitative Cardiac Center
Cedars-Sinai Heart Institute
Los Angeles, California USA
merz@cshs.org
Bernadine P. Healy, M.D.
•
•
•
•
•
EDITORIAL
The Yentl Syndrome
Bernadine Healy, M.D.
N ENGL J MED 1991; 325:274-276
Yentl, the 19th-century heroine of Isaac Bashevis
Singer's short story, had to disguise herself as a man to
attend school and study the Talmud. Being "just like a
man" has historically been a price women have had to
pay for equality. Being different from men has meant
being second-class and less than equal for most of
recorded time and throughout most of the world. It may
therefore be sad, but not surprising, that women have all
too often been treated less than equally in social
relations, political endeavors, business, education,
research, and health care.
Problem: Adverse Mortality Gap Resulting in a New Female
CVD Majority (National Center for Health Statistics and
American Heart Association)
Current Strategies Not Working Optimally in Women
Disparities in CVD Treatment for
Women
• 35,835 pts with NSTEMI: 41% women
• Women had:
DM, HTN, age; CAD events
Early ASA, heparin, GPIIb-IIIa, ACE-I
Revascularizations: CABG 41%
Discharge ASA, beta blocker, ACE-I,
statins (Four Magic Pills)*
• Death, MI, CHF
•
•
•
•
* Associated with a 90% reduction in recurrent major adverse cardiac events
Blomkalns AL et al. CRUSADE NSTEMI database. J Am Coll Cardiol. 2005;45:832-837.
Sex and Gender Differences in CVD
Terminology:
• Sex = biological sexual differentiation,
(e.g. women have ovaries, men have
testes)
• Gender = socio-cultural attributes of the
biological sex, e.g. women have
complex social networks, men have
wives
Sex and Gender Differences in CVD
More Terminology:
• Sex genotype = XX chromosomal makeup, e.g.
XX dictates ovarian development of stromal cells
in utero.
• Sex phenotype = genotype expression given the
certain conditions, e.g. premenopausal women
higher estrogen levels due to ovulation;
postmenopausal women have lower estrogen
levels due to no ovulation. Both are XX
genotype but differ in phenotypic expression.
Sex and Gender Differences in CVD
• Sex differences in perception = women have
greater perception (high frequency non-auditory
brain testing). Gay men are intermediate
between women (higher perception) and men
(lower perception), suggesting that this may be
genotypic1
• Sex differences in pain = women have lower
thermal pain thresholds compared to men.
Thresholds appear mediated by estrogen
levels, with higher E2 levels associated with
enhanced pain, suggesting that this may be
phenotypic2
1Shaywitz
et al, Nature 1995;373:607; 2 Fillingim et al, Pain Forum 1995;4:209
Sex and Gender Differences in CVD
• Gender differences in reporting = women are
more comfortable discussing feelings with friends
and reporting symptoms to physicians1, possibly
due to gender-related acculturation
• Gender differences in physician response to
symptoms = physicians are more likely to
evaluate men compared to women and
minorities2, possibly due to gender-related
presentation styles, and/or cultural sexism/racism
biases
1 Stoverink
J Fam Pract 1996;43:567
Sex and Gender Difference in CVD
Consequences of Sex and Gender Symptom Issues:
• If women perceive chest pain sooner after the onset
of ischemia/MI, this will lead to “longer” estimated
“ischemia onset” times in the ED, potentially leading
to conclusions that “women delay seeking
treatment”1, as well as making more women
“ineligible” for thrombolytic therapy. These may
contribute to more adverse outcomes.2
• If women report generally more symptoms suggestive
of chest pain, it will be a less effective diagnostic tool,
e.g. less specific for epicardial disease3. This may
lead to physician lack of confidence in testing, and
may also suggest that chest pain symptoms may be
difficult to optimize as a diagnostic tool.
1 Meischke Ann
Emerg Med 1993;22:1597; 2Vaccarino, Ann Int Med 2001;134:173; 3 Diamond NEJM 1979;300:1350
Potential Explanations for
Disparities in CVD Treatment in
Women
• Blame the victim – women do not seek healthcare
for symptoms and/or delay seeking attention
• Ageism – women are older on average and older
patients are less aggressively treated
• Sexism (medical judgment) – women are less likely
to have and/or die from CAD
• Biological sex differences in CVD – women more
often present with “female-pattern” disease, which
is not recognized compared to “male-pattern”
disease
Potential Explanations for
Disparities in CVD Treatment in
Women
• Blame the victim – women do not seek healthcare
for symptoms and/or delay seeking attention
• Ageism – women are older on average and older
patients are less aggressively treated
• Sexism (medical judgment) – women are less likely
to have and/or die from CAD
• Biological sex differences in CVD – women more
often present with “female-pattern” disease, which
is not recognized compared to “male-pattern”
disease
Gender Differences in Healthcare Seeking in the ED
for CV Symptoms: Women and men report CV
symptoms with same frequency
McKinlay JFl, J Health and Social Behavior 1996;37:1
Gender Differences in ED Care for CV Symptoms: Women receive
less assessment for CV symptoms
McKinlay JFl, J Health and Social Behavior 1996;37:1
Potential Explanations for
Disparities in CVD Treatment in
Women
• Blame the victim – women do not seek healthcare
for symptoms and/or delay seeking attention
• Ageism – women are older on average and older
patients are less aggressively treated
• Sexism (medical judgment) – women are less likely
to have and/or die from CAD
• Biological sex differences in CVD – women more
often present with “female-pattern” disease, which
is not recognized compared to “male-pattern”
disease
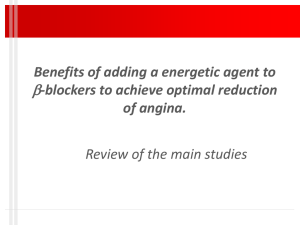
Sex and Myocardial Infarction (MI) Mortality:
Largest Gaps in Young Women
Hospital Mortality (%)
30
25
20
15
Women
10
Men
5
0
Men
Men
Women
Women
Overall
<50
50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89
Age (years)
Vaccarino V et al. NRMI. N Engl J Med. 1999;341:217-225.
Potential Explanations for
Disparities in CVD Treatment in
Women
• Blame the victim – women do not seek healthcare
for symptoms and/or delay seeking attention
• Ageism – women are older on average and older
patients are less aggressively treated
• Sexism (medical judgment) – women are less likely
to have and/or die from CAD
• Biological sex differences in CVD – women more
often present with “female-pattern” disease, which
is not recognized compared to “male-pattern”
disease
Paradox: Pathophysiological
Gender Differences: FRISC II
• 749 women and 1,708 men with
unstable coronary artery disease
• Entry criteria = symptoms plus
ischemia, defined as ECG change or +
enzymes
• Randomized to early invasive versus
noninvasive strategy
• Women were older, had fewer prior MI,
better LVEF and lower troponin T levels
Lagerqvist et al, JACC 2001;38:41
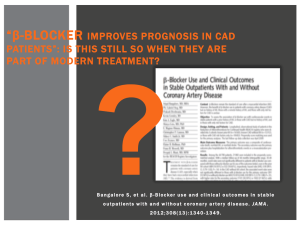
Women are less likely to have obstructive
CAD BUT equally/more likely to die
FemaleWomen
Male Men
EF 45%
12%*
14%
No CAD
25%*
10%
LM/3 VD/2
VD/2 prox LAD
Noninvasive
(Death/MI)
Invasive
(Death/MI)
32%*
43%
11%
16%
12%
11%**
*p<0.05 vs men; ** P = 0.001 vs noninvasive
Lagerqvist et al, JACC 2001;38:41
Potential Explanations for
Disparities in CVD Treatment in
Women
• Blame the victim – women do not seek healthcare
for symptoms and/or delay seeking attention
• Ageism – women are older on average and older
patients are less aggressively treated
• Sexism (medical judgment) – women are less likely
to have and/or die from CAD
• Biological sex differences in CVD – women more
often present with “female-pattern” disease, which
is not recognized compared to “male-pattern”
disease
Paradox: Women have a two-fold increase in “normal”
coronary arteries in the setting of ACS, nonSTE and
STE AMI
Bugiardini and Bairey Merz JAMA 2005;293:477-84
Female-pattern
Ischemic Heart
Disease
Microvascular Coronary
Disease (MCD)
Angina
Abnormal SPECT
No obstructive CAD
Abnormal coronary flow reserve
and elevated LVEDP
Diffuse atherosclerosis
by IVUS
NCDR estimate 3 million
women in the US – a larger
problem than breast cancer.
Circulation. 1999;99:1774
Female-pattern IHD is Associated with
Increased Risk of Major Adverse CV
Events: NHLBI WISE Study
30
25
20
A ll Wo m e n, N =19 0 ,
p( t re nd) =0 .0 3
% Wit h
M a jo r 15
E v e nt
N o C A D , N =15 3 ,
p( t re nd) =0 .0 3
10
5
0
0 .5 8 <2 .2 3
Pepine JACC 2010
2 .2 3 <2 .7 0
CFR
_
> 2 .7 0
Challenges for Women With IHD
●Delays in symptom recognition and
treatment
●Misdiagnosis
●Lower use of angiography, revascularization, aspirin, beta
blockers, statins, agiotensin-converting enzyme inhibitors
(ACE-I)(4 Magic Pills)*
●Less counseling and risk factor control
●Fewer referrals to cardiac rehab;
more “drop-outs”
●Lower adherence to proven guidelines (ACC/AHA, NCEP,
JNC VII, etc)
↑ Mortality
* Associated with a 90% reduction in recurrent major adverse cardiac events
The Yentl Syndrome
is Alive and Well
in 2011 Bairey Merz, EHJ 2011
→
Men > women with
with recognized
angina/ACS
The Yentl Syndrome
is Alive and Well
in 2011 Bairey Merz, EHJ 2011
→
Men > women with
with recognized
angina/ACS
→
Men > women go to
coronary
angiography
The Yentl Syndrome
is Alive and Well
in 2011 Bairey Merz, EHJ 2011
→
Men > women with
with recognized
angina/ACS
→
Men > women go to
coronary
angiography
→
Men > women receive
guidelines Rx
The Yentl Syndrome
is Alive and Well
in 2011 Bairey Merz, EHJ 2011
→
Men > women with
with recognized
angina/ACS
→
Men > women go to
coronary
angiography
→
Men > women
receive
guidelines Rx
→
Women > men death
What is the Answer?
• What is the Problem?
•
•
•
•
Lack of patient response to symptoms?
Provider sexism (medical judgment)?
Ageism?
Lack of knowledge and recognition of femalepattern ischemic heart disease resulting in
failure to use guidelines therapy?
What is the Answer?
• What is the Problem?
•
•
•
•
Lack of patient response to symptoms?
Provide sexism (medical judgment)?
Ageism?
Lack of knowledge and recognition of femalepattern ischemic heart disease resulting in
failure to use guidelines therapy
How to Get Results
• Re-name it “Ischemic Heart Disease (IHD)
rather than “Coronary Artery Disease
(CAD)”
• Use a simplified approach to IHD
management helps to increase adherence
to guidelines
• This can be achieved using an ABC format
to present important pharmacologic
therapies and lifestyle approaches
Know Your ABCs
• A
• Antiplatelets/anticoagulants*
• Angtiotensin-converting enzyme (ACE)
inhibitors/angiotensin-receptor blockers
(ARBs)*
• Antianginals
• B
• Blood pressure control
• Beta-blocker*
• C
• Cholesterol management (statin)*
• Cigarette smoking cessation
* 4 Magic Pills
What About Women (and Men) with
Female-Pattern Ischemic Heart Disease?
• Remember, ACS/angina guidelines are
not “cath” based – treat evidence of
ischemia and angina, not the cath
• Abundant evidence exists documenting
lifesaving risk reduction of the 4 magic pills
(ASA, ACE, BB, statin)
• The power of the prescription pen to
implement guidelines therapy
preferentially saves women’s lives
Clinical Practice Guidelines
•
This slide set was adapted from the following 2004-6 ACC/AHA
guidelines:
•
•
•
Cardiovascular Disease Prevention in Women 2004, 2007, 2010
Management of Patients With ST-Elevation Myocardial Infarction
Management of Patients with Unstable Angina and Non-ST-Segment
Elevation Myocardial Infarction
Preventing Heart Attack and Death in Patients with Atherosclerotic
Cardiovascular Disease
Management of Patients with Chronic Stable Angina
Update for Coronary Artery Bypass Graft Surgery
Evaluation and Management of Chronic Heart Failure in the Adult
•
•
•
•
•
•
The full-text guidelines and executive summaries are also available on
the
ACC and AHA websites at www.acc.org and www.americanheart.org
ACC=American College of Cardiology,
AHA=American Heart Association
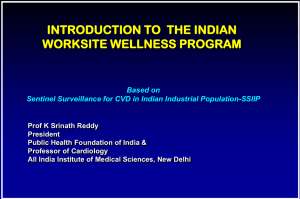
Impact of AHA Get With The Guidelines-CAD
Program on Quality of Care
Q1
Baseline
100
90
80
70
60
50
40
30
20
10
0
97 97
9395 96
83
79
8787
Q4
91
64656567
Aspirin
Q3
Q2
68
737574
70
67
Beta Blocker ACE Inhibitor
GWTG-CAD: 123 US Hospitals n=27,825
Labresh, Fonarow et al. Circulation 2003;108:IV-722
70
7675
82
57
Lipid Rx
Smoking
Cessation
Guideline
Implementation and
ACS and the
Sex Survival Gap
Novak et al Am J Medicine 2008;121:602.
Guideline
Implementation and
ACS and the
Sex Survival Gap
Following guideline
implementation,
mortality for women
improves and
the sex gap narrows
(RED)
+
Novak et al Am J Medicine 2008;121:602.
Guideline
Implementation and
ACS and the
Sex Survival Gap
Following guideline
implementation,
mortality for women
improves and
the sex gap narrows
(RED)
Persistent sex gap
(BLUE)
suggests more work
still needed
to understand sexspecific
pathophysiology
to improve outcomes
for women and men
+
Novak et al Am J Medicine 2008;121:602.
WISE-ISCHEMIA:
A Companion Trial to the
NHLBI-sponsored ISCHEMIA
Noel Bairey Merz MD
Carl Pepine MD
Harmony Reynolds MD
Leslee Shaw PhD
Eileen Handberg PhD
Rhonda Cooper-DeHoff PharmD
John Spertus MD
David Maron MD
Judy Hochman MD
Women’s Ischemia
Syndrome Evaluation
WISE
International Study of
Comparative Health Effectiveness
with Medical and Invasive
Approaches
1615PC Bairey-Merz/Slide39#
Figure 1. ISCHEMIA-WISE
Companion Trial to ISCHEMIA
ISCHEMIA
Enrolled patients
n=8650
C
C
T
A
LM
no
obstructive
CAD
(US/Canada)
ISCHEMIA - type
Patients sent to
cath lab clinically
(evidence of
ischemia)
C
A
T
H
Randomized in
main trial
n=8000
no
obstructive
CAD
excluded
No obstructive CAD
by ISCHEMIA CCTA
n ~ 250-400
WISE – ISCHEMIA
Randomized trial
n=2600
No obstructive CAD
by clinical invasive
coronary
angiography
n= 2200-2350
Obstructive CAD
excluded
Atherothombotic
Strategy
Atorvastatin
40-80 mg
daily
Aspirin
81-325mg
daily
Hypertension /
Angina Strategy
Step 1
• Metoprolol 50400mg or
Verapamil SR
240-480mg if
metoprolol
intolerant daily
Continued
Angina Strategy
Step 1
• Isosorbide
mononitrate
30-120mg
daily
Step 2
Step 2
• Add ramipril
2.5-20mg daily or
losartan 50-100mg
daily for ramipril
intolerant
Step 3
• Add HCTZ
12.5-25mg daily
• Add
ranolazine
500-1000mg
twice daily
Problem: Adverse Mortality Gap Resulting in a New
Female CVD Majority (National Center for Health Statistics and American
Heart Association)
Deaths in Thousands
520
500
480
460
NHLBI WISE
Study
And Guidelines
Campaigns
440
420
400
3800
79 80
85
90
95
Years
Males
Females
00
04
Problem: Adverse Mortality Gap Resulting in a New
Female CVD Majority Solution: Clinical Translational
Research and Guidelines
Deaths in Thousands
520
500
480
460
440
420
400
3800
79 80
85
90
95
Years
Males
Females
NHLBI WISE
Study, NHLBI
and AHA Red
Dress
Awareness
and Guidelines
Campaigns
00
04
Summary: Women and Heart
Disease
• Women face a higher mortality from IHD
due to their relatively higher prevalence of
“female-pattern” ischemic heart disease
• Application of guidelines therapy is
improving outcomes in women with IHD.
• Ongoing work is evaluating mechanisms
and interventions directed at sex
differences in IHD.
• Questions, comments, referrals?
merz@cshs.org