Congenital Myasthenic Syndromes (CMS)
advertisement
")
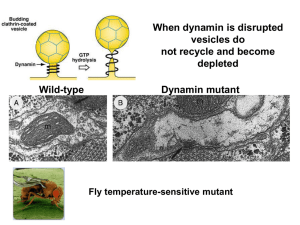
Congenital Myasthenic Syndromes Shahriar Nafissi, MD Associate Professor of Neurology Tehran University of Medical Sciences Physiology The Neuromuscular Junction Action Presynaptic potential channel terminal Ca2+ Ca2+ action potential opening voltage-gated Ca2+ channels ↑Ca2+ permeability Ca2+ Presynaptic Ca2+ terminal channel ACh ↑Ca2+ Ach release from synaptic vesicles Synaptic cleft Na+ ACh Na+ Receptor molecule ACh binding to Ach receptors opening ligand-gated Na+ channels. Na+ Action potential Na+ Action potential ↑Na+ permeability depolarization action potential generation in the postsynaptic membrane ACh Choline Acetic acid ACh receptor site Acetylcholinesterase Ach →acetic acid + choline ▲ Ach-Esterase Presynaptic terminal ACh Acetic acid Synaptic vesicle Choline ACh Choline in the presynaptic terminal Choline + acetic acid → Ach → Synaptic vesicles Structural Reality By John Heuser and Louise Evans University of California, San Francisco Ligand- Gated Ion Channel 2α + β + ε + δ Congenital Myasthenic Syndromes • Group of diseases caused by genetic defects affecting neuromuscular transmission • Heterogeneous inheritance and pathophysiology Classification • Presynaptic Defect – Choline Acetyl Transferase deficiency – Paucity of synaptic vesicles – Lambert-Eaton like CMS • Synaptic Defect – Endplate ACh Esterase deficiency • Postsynaptic Defects – – – – – – Kinetic abnormality of AChR AChR deficiency Rapsyn Dok-7 SCN4A MuSK • No identified Defect percentage of CMS subtypes in different centers Diagnostic Clues in CMS • Weakness/fatigability of limbs and oculobulbar muscles • Early onset (since neonatal period) • Positive family history • EDX findings (RNS, SFEMG) • Response to anti-cholinesterases • Absence of anti-AChR, MuSK , VGCC antibodies Diagnostic Difficulties • Diagnostic problems – – – – – – Late onset (in adult) No response to anticholinesterases No family history Episodic symptoms No ophthalmoplegia or cranial involvement Decrement may not be present in all muscles, or present only intermittently • Misdiagnosed as – congenital myopathy – Seronegative MG (late onset) – Metabolic myopathies R ABD POLL BR EVIS Ampl (mV) over Study 5.0 2.5 0.0 1 24 Yo, referred as congenital myopathy Responsive to Mestinon 2 3 4 Electrodiagnosis • Decrement after 2-3 HZ RNS – Absent in ChAT def., Na-Channel CMS, Some cases of Rapsyn • If negative, try higher frequencies • Try conditioning with 5 minutes 10HZ stimulation • Single-Fiber EMG Electrodiagnostic clues • Repetitive CMAP after single stimulus • Low amplitude CMAP with significant increment after high frequency RNS • Response to Tensilon test Presynaptic Syndromes Choline-Acetyl Transferase deficiency (ChAT def.) • ± neonatal hypotonia, gradually improve • Attacks of apnea, bulbar paralysis precipitated after infection, fever, excitement • No symptoms or mild-myasthenic symptoms between attacks • Reduced number of attacks with increasing age • Treatment: – AchE Inh. for myasthenic symptoms and prophylaxis – IM AchE Inh. Injection on crisis Synaptic Defect Endplate ACh Esterase deficiency AChEsterase Clinical Features • Myasthenic symptoms since birth or early childhood • delayed milestones • Weakness facial, axial, limb± ophthalmoplegia • Fatigable lordosis and scoliosis • Finger extensor weakness • Slow pupillary light response •11 yo, weak since infancy with ptosis, restricted EOM, sluggish pupillary reflex, lordosis •Worsening with Mestinon, some response to pseudoephedrine Decrement after 3 HZ RNS Repetitive CMAP after single stimuli Catalytic Subunits Collagen Tail Formed by triple-helical association of three collagen strands (ColQ) Therapy • AchE inhibitors ineffective • Increased muscarinic side effects • Some improve with ephedrine or pseudo-ephedrine 20 yo, Ptosis since infancy Delayed walking, Ophthalmoparesis generalized weakness No reponse to mestinon, 3,4-DAP, Quinidine, fluoxetine Improved with ephedrine Mutation found in ColQ L ABD DIG MIN (UL) 1.1 1.2 1.3 Ampl (mV) over Study 1.4 10 1.5 1.6 5 1.7 2 0 1.8 1.9 1 2 3 4 5 1 3 5 4 1.10 30ms 2mV 16 yo, Lordotic gait from beginning, WCB from 11 No ptosis or ophthalmoparesis proximal > distal Diagnosed as DMD AChRAb negative Worse with Mestinon R ABD POLL BREVIS 1.1 1.2 1.3 1.4 1.5 1.6 2 1.7 1.8 1.9 1 5 3 1.10 30ms 500µV 4 R ULNAR - ADM R MEDIAN - APB 2 2 1 3 5 4 Wrist 1 30ms 5mV 16mA 14-33% decrement 1 Wrist 1 30ms 1mV 20mA Repetitive CMAP 2 2 1 3 4 5 B.Elbow 2 30ms 5mV 16mA 1 3 El bow 2 30ms 1mV 20mA Post-Synaptic Syndromes Post-Synaptic Syndromes • Kinetic abnormalities of AChR – Slow-Channel Syndrome – Fast Channel Syndrome • Low-Expressor AChR Deficiency • Rapsyn Deficiency • Sodium-Channel Myasthenia • Dok-7 Synaptopathy Slow-Channel Syndrome • Autosomal Dominant • Selective weakness of cervical, scapular, finger ext., • Eye movements: spared or mildly affected • Early onset: gradually progressive • Late onset and mild • Fluctuating • Severely affected muscles become atrophic • EMG – Repetitive CMAP after single stimuli – Decrement only in weak muscles • Pathogenesis – Prolonged AChR opening ↑ cations and Ca++ Ca++ excess activation of protease, lipase, free radicals endplate myopathy – Depolarization block Family M. Slow channel G153S Intra familial variability for severity mild severe • Pathology: tubular aggregates • Genetics: mutation in AChR subunits • D.D.: •Polyneuropathy •Motor Neuron Disease •Radial palsy •Mitochondrial disease •Limb-Girdle MD •Myotonic Dystrophy •FSHD Therapy • AChE Inh. Ineffective or only temporary improvement • Probably accelerate progression by cationic overload • Long-lived open channel AChR blockers – Quinidine 200 mg × 3-4/d – Fluoxetine 80 mg/d Ach Receptor Deficiency ε/ Low-Expressor AChR mutations • Reduced AChR expression to < 15% • Mild to severe phenotype • Most cases mutation in ε-subunit of AchR fetal AchR harboring γsubunit is substituted • Mutations in both alleles of a non-ε subunit incompatible with life • Most respond well to AChE Inh ± DAP •18 yo, referred as MG for a consult before rhinoplasty •Has always been weak in physical activity and if doing so, fatigued very fast. •Fluctuating ptosis and diplopia. •Stable and non-progressive during these years and worse in the evening •Significant subjective and objective improvement with Mestinon • Myasthenic symptoms since infancy • Very good response to mestinon • Both have been misdiagnosed as myasthenia gravis and both thymectomised • Mutation in CHRNE ( ε-subunit of AchR) Rapsyn Tyrosine kinase function : AChR concentration and linkage to cytoskeleton Rapsyn Deficiency • Has a crucial role in concentrating AChR in post-synaptic membrane • Birth or neonatal ± Arthrogryposis • Sometimes juvenile-adult onset • Facial deformity: prognathism, malocclusion • Severe masticatory weakness • Ptosis without ophthalmoparesis • Cervical, truncal, limb usually spared • Stable and benign course • EMG – Decrement not present in all – Single-Fiber EMG • Partial to well response to AChE Inh • Addition of 3,4-DAP sometimes beneficial DOK7 Synaptopathy Dok-7 interacts with MuSK and is essential for postsynaptic specialization of the neuromuscular junction DOK7 Synaptopathy Clinical features • Difficulty in walking developing after normal motor milestones • Proximal muscles weakness > distal • Ptosis often present, EOM rarely involved • EMG always abnormal – decrement in amplitude and/or – jitter and blocking on single-fiber studies • No benefit from anticholinesterase, sometimes worsened • Responded to ephedrine Clinical clues pointing to a specific diagnosis Endplate AChE deficiency ● Repetitive CMAPs ● Refractoriness to cholinesterase inhibitors ● Delayed pupillary light reflexes Slow-channel CMS ● Repetitive CMAPs ● Selectively severe involvement of cervical and wrist and finger extensor muscles in most cases ● Dominant inheritance in most cases Clinical clues pointing …-2 Endplate choline acetyltransferase deficiency ● Recurrent apneic episodes ● No or variable myasthenic symptoms between acute episodes ● EMG decrement at 2-3 Hz can be absent at rest but appears after stimulation at 10 Hz for 5 min, then disappears slowly. Rapsyn deficiency ● Multiple congenital joint contractures ● Increased weakness and respiratory insufficiency precipitated by intercurrent infections ● EMG decrement can be mild or absent. Dok-7 myasthenia ● Proximal greater than distal limb weakness, ● mild ptosis, and normal ocular ductions in the majority ● May deteriorate on exposure to pyridostigmine Standard pharmacotherapy • ChAT deficiency: AChEI oral prophylaxis, parenteral use in crisis • Achesterase deficiency: avoid AChEI; try ephedrine • AChR deficiency: AChEI; 3,4-DAP also helps in 30–50% • Slow-channel CMS: quinidine or fluoxetine • Fast-channel CMS: AChEI and 3,4-DAP • Rapsyn deficiency: AChEI; some benefit further from 3,4-DAP • Limb-girdle myasthenia: AChEI; some benefit from ephedrine • Dok-7: ephedrine ?