The Child with Respiratory
Problems
Acute Otitis Media
An infection of the middle ear cavity most common in
healthy children between 6 months & 2 years. 8590% of all children has at least one episode before
school age. Incidence increases in winter months,
boys>girls, higher in families with smokers, daycare
attendance, cleft palate, Down Syndrome.
Often proceeded by a URI or allergy, which results in
edema and congestion of the mucosa of nasopharynx,
eustacian tubes and middle ear leading to eustacian
tube dysfunction.
Etiology of OM:
Can be a bacterial infection, but most often viral.
– Contributing factors:
• In children, eustacian tubes are short, wide and straight, lying
relatively horizontal.
• Abundant pharyngeal lymphoid tissue readily obstructs tube
• Usual lying down position favors pooling of fluids, ex., formula in
pharyngeal cavity
• Most common organisms are: streptococcus pneumoniae,
haemophilus influenza and viruses
• Organism gains access when normal patency of tube is blocked.
Air trapped in middle ear is reabsorbed, creating negative pressure
allowing reflux of bacteria, viruses.
• Bacteria, viruses + obstruction of flow of secretions leads to middle
ear effusion (fluid).
Clinical Manifestations:
Rhinorrhea, malaise, irritability, restlessness, pain in the ear,
pulling or tugging at the ear, purulent discharge, diarrhea or
vomiting, fever 102 or higher (common, but not universal
symptom), vertigo, loss of appetite, enlarged post auricular and
cervical lymph nodes.
Tympanic membrane is normally translucent, pearly, pin/gray.
With OM, TMintense erythema, bulging toward examiner,
immobile with loss of identifiable landmarks (short process,
handle of malleus and reflex) However, hyperemia (redness)
of TM also occurs from crying, fever.
Discharge from ear perforation of TM with acute relief of pain
Treatment and Nursing Care
If suspected bacterial infection: Amoxicillin for 10 days,
reexamine TMs. If no improvement in 48 hrs. dosage may be
increased, or different abxs tried.
Many PMD’s are now opting not to treat OM as most (<90%) are
viral infections.
Auralgan otic solution if TM is not perforated for comfort. Teach
parents how to instill eardrops. <3 years, pull pinna down and
back, instill drops straight into canal – do not warm solution,
use at room temperature – let child lie with affected ear up
for several minutes.
Do not use antihistamines in young children thicken secretions
and may cause systemic complications. Parent can use
Dimetapp for decongestion to allow child to sleep.
TX/ NSG Care cont..
Children’s Tylenol or Ibuprofen for fever >102
Teach parents need for follow up care, repeated or incompletely treated OM can &
WILL lead to hearing deficits.
Long term complications of AOM – conductive hearing loss. AOM with effusion –
sensorineural hearing loss
Teach parents not to put child to sleep with a bottle.
Recurrent infections (3 episodes in 6 months or 2 episodes in <6 months or 4 episodes
/year – may be treat with prophylactic abx at ½ dose of amoxicillin at bedtime in
winter and early spring.
If prophylaxis fails: myringotomy with placement of tympanostomy tubes – for
persistent middle ear effusion (collection of fluid in middle ear). Allows for
ventilation and drainage, Eustachian tube healing.
Parent teaching
Teach parents tubes will “come out” on their
own, child must not put his head under water
in shower, bath or swimming.
If TM is ruptured (parent reports child suddenly
has not pain and there is drainage from ear),
tell parent to wipe drainage with clean gauze
or cloth. Topical abs otic suspension may be
given. Teach installation of drops.
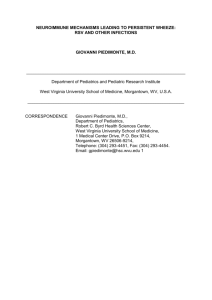
Healthy TM
Bulging TM
Acute OM
OM with effusion
Perforated TM
Tubes
Bronchiolitis
RSV (respiratory syncytial virus)
•
•
•
•
Rare >2 years,
VERY common winter/spring,
Common respiratory illness of young children,
Associated with exposure to adults with URIs
and daycare.
Clinical Manifestations:
• If it is Oct/Nov and young child (under 2) presents with runny
nose, cough, fever
THINK RSV
• Rhinorrhea, sneezing, cough, low-grade fever followed in
several days by tachypnea and wheezing from inflammation of
small airways.
• Inflammation leads to trapped air (hyperinflation)
• Plugging of small airways with mucus and debris
• Signs of acute respiratory distress: nasal flaring, tachypnea,
intermittent cyanosis, retractions, prolonged expiratory phase
caused by hypoxemia, tracheal tug
Dx: RSV cultures from nasal secretions rapid test/ viral cx
Tx/ Nursing Care
Bronchodilators (Proventil) by nebulizer, Solu-Medrol
(corticosteroid) IV, Tylenol or Motrin for fever.
Croup or mist tent: Teach parents, tent must stay
closed, change child’s clothes often because they will
become damp from moist, cool atmosphere
Ribavirin aerosol – antiviral agent given by nebulizer
for high-risk children (congenital cardiac or
respiratory problems) *Drug is teratogenic – high risk for pregnant staff
or mother*.
RSV globulin/Synagis
• RSV globulin for preemies at high risk, administered
monthly by IV infusion during winter months.
• Synagis, an antibody solution given by IM monthly
(November-march) , few side effects except pain and
transient redness at site.
– Both are very expensive, not all insurance company’s will
pay for them.
Treatment
• In healthy child, RSV/Bronchiolitis resolves in
7-10 days may be treated at home if no
respiratory distress present.
Acute Epiglottitis
• ETIOLOGY: An obstructive inflammatory
process principally occurring in children ages
2-5 years, but can occur from infancy to
adulthood.
True medical emergency.
• Usually caused by haemophilus influenza
bacteria (Hib) and can be virtually eliminated
(95% reduction) by Hib vaccine given at 2 - 4,
6 months and a booster at 12-15 months.
Upper Airway Anatomy
.
• PATHOLOGY: fulminate, abrupt onset with
rapid progression. Usually preceded by a sore
throat, less often by cold symptoms. Child
usually awakens with sore throat and pain on
swallowing. Fever, pulse, respiration – child
is sicker than clinical findings suggest and
looks worse than he or she sounds.
Presentation
• Classic diagnostic picture: “tripod position” child insists on
sitting upright and is leaning forward with chin thrust out and
mouth open with tongue protruding, drooling from pain of
swallowing saliva
• Absence of spontaneous cough, “toxic” looking appearance,
extreme restlessness (air hunger), irritability
• Child has an anxious, frightened expression
• Voice is thick, muffled with a frog-like croaking sound on
inspiration, but not hoarse
• May have supra and substernal retractions, mild hypoxia to
frank cyanosis may be present.
• Throat is red and inflamed with cherry red epiglottis and a
classic “thumb nail” sign on lateral x-ray.
Nursing Interventions
• Never force child to lie down, can lead to complete airway obstruction.
• Never visualize throat, no tongue depressors or throat cultures. Throat
should be examined only with anesthesiologist and intubation tray at
bedside. (preferably in the OR with full resuscitation equipment and
tracheotomy set available)
• Have child sit in parent’s lap , decreases anxiety, encourage slow, quiet
breathing which will provide better air exchange.
• NO IV’s or blood drawing
• Notify physician immediately and prepare an intubation tray. Child needs
to be intubated by nasotracheal tube before obstruction occurs. Call
anesthesia because he needs to be intubated while sitting up, should be
done in the OR, ideally.
• Have portable x-ray done, or MD who can perform immediate intubation or
tracheostomy should accompany if child must go to radiology.
Treatment after airway stabilization
• Treated with Ceftriaxone (Rocephin) 5075mg/Kg/day q12h. Produces rapid clinical
recovery; child can be extubated in 48-72
hours.
• Teach parents the importance of Hib vaccine.
Acute Laryngotracheobronchitis (LTB)
“Croup”
• ETIOLOGY: viral infection affecting
children <5 years, primarily toddlers, (range 3
mos-8 yrs). Usually preceded by a URI, which
descends to adjacent structures.
1 mm swelling of edema in the trachea,
bronchi of an infant or toddler closes
75% of their airway
Acute tracheoebroncitis “Croup”
• PATHOLOGY: gradual onset with low-grade fever, slowly
progressive respiratory stridor (hallmark sign) caused by child
struggling to inhale air past the obstruction (inflammation of
lining of larynx and trachea causing narrowing).
• Classic cough (barking or seal like) after several days of
coryza.
• Slight to moderate respiratory distress with mild wheezing,
non-toxic appearance, hoarseness of voice, lower rib cage
retractions to tracheal tug depending on severity of obstruction
• Irritable, restless
• Obstruction severe enough to cause inadequate exhalation of
CO2 causes respiratory acidosis and can lead to respiratory
failure.
Airway in croup
Treatment and nursing
interventions
• Children without stridor at rest can be treated
at home for mild croup with a cool air
vaporizer, which constricts edema – the effect
of mist therapy may be psychological.
• Allow child to drink any fluids, helps lessen
secretions
• For severe respiratory distress, >60 breaths per
minute, stridor at rest, retractions, difficulty
breathing must be hospitalized.
Treatment - Medical
1) Racemic epinephrine (nebulized) and alphaadrenergic drug mucosal vasoconstriction and
edema. Rapid onset of relief in 10-15 minutes.
May need to repeat q1-2 hours.
2) Solu-Medrol IVPB – anti-inflammatory agent,
edema. Takes approximately 6 hours for onset of
relief. Give for 12-24 hours for improvement (by
O2 sat and respiratory rate).
3) Proventil (bronchodilator) by nebulizer q2-4 hours
as needed.
Treatment - Nuring
• Continuously monitor O2 sat, pulse (tachycardia) and
respirations
• Signs of impending airway obstruction: pulse and
respirations, sub, suprasternal retractions, intercostal
retractions, flaring nostrils, tracheal tug,
restlessness.
• Child should be kept quiet and at rest. Reassure
parents who may be frightened by child’s appearance
(struggling to breathe). Recovery is generally
prompt.
Acute Spasmodic Larygitis, also
known as “midnight croup”,
• Less severe variant is viral, characterized by
attacks of laryngeal obstruction that occur at
night, common 1-3 years.
• Sudden onset, history of URI or previous
attack, familial, without signs of inflammation.
• Child awakens with barking, metallic cough,
hoarseness, dyspnea, inspiratory stridor,
restlessness, but afebrile.
• Child is frightened, anxious, prostrated.
Nursing interventions
• Treatment can be done at home: cool mist
from vaporizer, take child outside in winter or
into a cold garage, or open freezer door OR
warm mist from running hot water in bathroom
until spasm subside. Try either treatment for
30 minutes, if no improvement, take child to
ER, may be epiglottitis
• Usually benign, self-limiting disorder. If
severe respiratory distress, treat same as LTB.
Anatomy – Lower Respiratory
.
“
All that wheezes is
not asthma, but
asthma usually
wheezes.”
Reactive Airway Disease - Asthma
• ETIOLOGY: Considered an exaggerated response
to a respiratory trigger (antigen), possibly mediated
by immunologic factors, physical and chemical
stimuli, and viruses. Most common chronic disease
of childhood.
• PATHOLOGY: intermittent with symptom-free
periods with no meds or chronic with frequent or
continuous medical treatment needed.
– Characterized by: bronchospasm, secretion of mucus,
inflammation and edema of respiratory tree.
– Wheezing on expiration, dyspnea, SOB, course crackles
rhonchi. With increased severity wheezing may also be
heard on inspiration.
Presentation
• Children often experience a prodromal itching on
front of neck or upper back. May c/o headache,
feeling tired or “tight” chest, irritable, hacking,
paroxysmal cough, irritable and non-productive from
bronchial edema. Accumulated secretions cause
coughing.
• With production of mucus, cough becomes rattling
with thick sputum. Bronchial spasm size of airway
which can be occluded by a mucus plug.
• Hallmark diagnostic sign: coughing at night in the
absence of a respiratory infection. Disrupts sleep,
child suffers in school.
Presentation
• With a severe episode: an audible wheeze with
prolonged expiration as child tries to breathe more
deeply. Lips dark redcyanosis, also in nail beds
and skin, especially circumoral. Child sits up, is
anxious and frightened, diaphoretic. Speaks with
short, panting, broken phrases. Child may be
diaphoretic and refuse to lie down.
• Infants normally have a high respiratory rate making
this more difficult to diagnose. Lungs will be
hyperresonant (too much “old” trapped air). Problem
is not breathing in, but breathing out.
Anatomy – Distal Respiratory
Asthmatic Changes
Cautions - Asthma
• With severe spasm or obstruction, breath
sounds may become inaudible, cough is
ineffective, respiration increases respiratory
failure with imminent asphyxia.
• With airway rigidity (edema), wheezing will
be expiratory AND inspiratory. Systemic
steroids are needed.
• Not all asthmatics wheeze- be careful!
Treatment
• Treatment – very individualized. Assist child
to live as normal a life as possible. Prevent
exposure to allergen, if possible, ex. Cigarette
smokes, animal dander, dust mites, protein
foods (chocolate, strawberries etc).
Treatment goals
• Drug therapy – goal is to manage underlying inflammation. Use inhaled
steriods daily. Will prevent attacks by controlling inflammation, but is not
used for an acute attack. Must be used daily, by MDI (metered dose
inhaler), 2-4 weeks before effect takes place. Inhalers can be used with a
spacer for young children who cannot coordinate breathing and pressing on
inhaler.
• Proventil/Albutrerol (bronchodilator) by MDI – beta-adrenergic agonist
(mimics adrenaline/epinephrine). Used for acute exacerbations and for
prevention of exercise induced asthma.
• Singulair (leukotriene inhibitor) once daily, works by inhibiting reaction of
mast cells in respiratory tree to antigen, inhibiting IgE.
• Remember that an allergic reaction like asthma involves the immune
system response
Nursing interventions
• Teach child how to measure peak flow with a
meter. PEFR (peak expiratory flow rate)
measures flow velocity during a forced
expiration, varies according to child’s age,
height, sex. Child needs to establish his/her
“personal best” over a 2-3 week period, 3
times/day to establish a base line.
Peak Flow
PEFR is base on green, yellow, red colors to help child
remember.
Green zone = 80-100% of personal best. No symptoms present,
routine treatment plan can be followed.
Yellow zone = 50-80% of personal best signals caution. Acute
exacerbation may be present. Maintenance therapy may need
to be increased. Call health care provider if no improvement.
Red zone =below 50% of personal best signals a medical alert.
Severe airway narrowing may be occurring. Take immediate
bronchodilator. Notify provider immediately if PEFR does not
return and stay in yellow or green zone.
Child has pre-determined plan to follow based on above results.
Cystic Fibrosis
CF
• ETIOLOGY: a generalized dysfunction of
the exocrine glands (those that secrete
externally through a skin surface) that
produces a multisystem disorder. Inherited as
a recessive trait.
• PATHOLOGY: thick, sticky, tenacious
mucous secretions that obstruct the ducts of
exocrine glands
Clincal Manifestations
• Newborn: meconium ileus (thick, tar-like) may cause
intestinal obstruction requiring surgery
• Child has frequent, recurrent pulmonary infections: bronchitis,
pneumonia and ultimately COPD caused by obstruction of
respiratory tract with thick, tenacious secretions
• Malabsorption syndrome: failure to gain weight, distended
abdomen, thin arms and legs, lack of subcutaneous fat from
inability of pancreatic enzymes to reach digestive tract
resulting in impaired digestion and absorption of nutrients.
• Steatorrhea: bulky, foul-smelling, frothy, fatty stools
predisposes to rectal prolapsed
Clinical manifestations
• Sexual development: boys sterile due to
aspermia, girls difficulty conceiving and
bearing children (from increased viscosity of
cervical mucus which acts as a plug and blocks
entry of sperm)
• Parent will generally report that child “tastes
salty”. Sweat test reveals high sodium and
chloride levels in sweat, a symptom unique to
CF
Treatment
• Treatment involves controlling symptoms, not
cure. Postural drainage morning, between
meals, before bedtime to loosen respiratory
secretions.
• High fluid (Gatorade) intake to decrease
viscosity of secretions, prevent dehydration
and electrolyte imbalances. Exercise such as
swimming increases lung capacity.
Treatment
• Nebulizer treatments with Bronchodilators,
mucolytics, expectorants. Child may sleep in a
mist tent.
Nursing interventions
Prevent infection
•
•
•
•
•
•
Prophylactic abx
avoid people with URIs
report any URIs immediately
adequate nutrition
Genetic counseling
Diet: fat, protein, calories. Administer fat-soluble
vitamins A, D, E, K, multivitamins, iron. Extra slat to
compensate for losses, especially in hot weather.
Nursing interventions
• Administer pancreatic enzyme before every meal and
every snack to enhance absorption of fats. Tablets or
powder (mix powder with cold food ex. applesauce)
approximately 30 minutes before eating. Dose
depends on condition of stools.
• Teach child-increasing responsibility for own
treatment, diet, meds, etc.
• Encourage verbalization of anger or frustration at
being “different”.
• Refer parent and child to Cystic Fibrosis Foundation
center and local support groups
Pneumonia
• ETIOLOGY: a common childhood disease
occurs more frequently in infancy and early
childhood as a primary infection or a
complication of other diseases.
• PATHOLOGY: Classified as either lobar
(large segment of one or more lobes),
interstitial (confined mostly to alveoli) or
bronchial (confined to terminal bronchioles)
depending on anatomic site in respiratory tree.
Pneumonia - Types
2 types: viral and bacterial
Viral pneumonia occurs more frequently than
bacterial, often associated with URIs and RSV
disease. Although less severe, viral infections
can lead to secondary, superimposed bacterial
infection because of damage to mucosa.
Signs and symptoms
• fever, generally over 102, cough, unproductive to productive
with whitish sputum, tachypnea
• breath sounds can include rhonchi, fine crackles, dullness to
percussion, chest pain often exaggerated by deep breathing,
retractions, nasal flaring, pallor to cyanosis
• Bacterial pneumonia can also cause chills, and referred pain to
the abdomen. Child appears very ill with rapid, shallow
respirations, malaise. May also exhibit signs of meningeal
irritation (CNS) with irritability, restlessness, lethargy
• Children also may have vomiting, diarrhea
• Most children can be treated at home if respiratory distress is
not present.
Treatment
nursing care& nursing interventions
• Antibiotic therapy, oxygen, fluids, chest PT, Tylenol or Ibuprofen for fever
reduction.
• Administer antitussives (cough medicines) if cough is disturbing and won’t
allow child to rest or sleep. Monitor I&O, vital signs, breath sounds
frequently. Young infants and toddlers may need suctioning of secretions
with a bulb syringe in their nostrils.
• Plan nursing care so child can rest.
• May be in a cool mist tent to help moisten the airways and provide oxygen
(change clothes frequently because of dampness)
• If child is isolated, provide for family visiting and diversional activities to
reduce psychological stress which makes breathing more difficult.
• Child may lie in any position, but is usually more comfortable in low
Fowler’s, or lying on affected side of chest which helps splint chest when
coughing
Parent teachings
• Although bacterial pneumonia takes longer to
resolve, prognosis is generally good, 7-10
days.
• Teach parents importance of vaccination
available to prevent pneumococcal disease:
(Prevnar) one of the most common types of
bacterial pneumonia, especially if child is in
day care.