lecture 7
advertisement

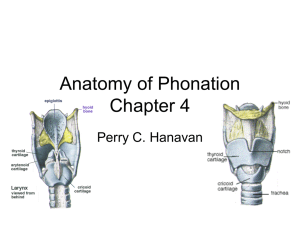
Neurogenic Voice Disorders 1 Innervation: Vocal Folds • Main Cranial Nerve: Vagus (X) -Divides into left & right branches, then further divides into 3 branches, 1) Pharyngeal 2) Superior laryngeal 3) Recurrent laryngeal 2 Vagus Nerve Branches Superior Pharyngeal Constrictor Muscle Nucleus Middle Pharyngeal Ambiguus Constrictor Muscle Jugular Foramen Pharyngeal Branch Vagus Nerve (x) Superior Laryngeal Nerve Inferior Pharyngeal Constrictor Muscle Recurrent Laryngeal Nerve 3 Pharyngeal Branch • Innervate pharyngeal middle constrictor • Subdivide & join branches from sympathetic trunk, external laryngeal & glossopharyngeal nerves= Pharyngeal plexus – Plexus supplies innervation to pharynx & muscles of velum • Lesions here result in: – adductor paralysis & velopharyngeal paralysis. 4 Superior Laryngeal Nerve Branches • Divide into internal & external branches 1) Internal laryngeal nerve: -Divides further: upper & lower branches – Both provide afferent info (sensory) 1. Upper: Supplies mucous membranes of epiglottis & vestibule of larynx 2. Lower: Motor supply to CT 2) External laryngeal nerve: – Controls cricothyroid muscle 5 Recurrent Laryngeal Nerve Branches • Divides into right & left 1) Right & left recurrent nerves: -Innervate all intrinsic muscles except the CT. -Involved in sensory supply of subglottic mucous membranes 6 Branches of Vagus & Result of Lesion • Pharyngeal Branch: muscles of velum (levator & levator veli palatini) are affected one or both sides. • Superior Laryngeal Branch: CT muscle affected on one or both sides. • Recurrent Laryngeal Branch: All intrinsic laryngeal muscles are affected unilaterally or bilaterally resulting in fixed abduction position. 7 Lesions & Disorders Causing Hypoadduction 1) Lesions that damage vagal nuclei within the brainstem or “intramedullary” -Lesion occurs after nerves leave the skull= “extracranial” -Damage before leaving the skull but outside the brainstem itself= “extramedullary” -All intra- & extramedullary and extracranial lesions occur before vagus separates into branches (RLN, SLN, pharyngeal) 8 Brainstem Lesions 1) Affecting nuclei of right and left vagus nerves: -results in bilateral paresis or paralysis of pharyngeal & laryngeal muscles, -affects sensory function, -both folds may be involved and are abducted -airway is without protection, -fortunately unilateral lesions occur more than bilateral. 9 Symptoms A) Unilateral lesions: • unilateral v.f. paralysis • breathiness and aphonia • tremorous vowel prolongation's • reduced loudness • reduced endurance • lowered pitch • diplophonia • hypernasal resonance • swallowing problems 10 Symptoms B) Bilateral lesions: • bilat. v.f. paralysis • open glottis • almost total absence of vibration • marked hypernasality • distorted pressure consonants • absent or weak cough • absent or weak gag reflex • dysphagia (nasal regurgitation on swallowing)11 Superior & Recurrent Laryngeal Nerve Lesions 1) SLN & RLN: -Do not create velar problems -Result in all of the preceding laryngeal symptoms listed -If the paralysis is complete, intracranial studies should be ordered by the physician 2) SLN alone or extracranial lesions: -Affect CT muscle and impact on pitch -Suspected when one fold lags in adduction 12 Symptoms: SLN Lesions • Loss of high pitches • Instability in the upper range • Breathiness and weakness 13 Bilateral SLN Paralysis Symptoms • Thyroid cartilage will not tilt on the cricoid cartilage during phonation • v.f.’s appear short • v.f.’s appear bowed • Epiglottis overhangs the anterior part of the v.f.’s • Breathy or hoarse quality • Reduced loudness • Ability to alter pitch is impaired • Singing is difficult 14 Inferior RLN Lesions • Result in paralysis of all intrinsic laryngeal muscles of the larynx with the exception of the CT • CT assumes a compensatory function and adducts • Folds may be positioned at midline or paramedian position rather than in an adducted position 15 Unilateral RLN Paralysis Symptoms • Reduced airway • Weak cough • Reduced loudness • Diplophonia • Pitch breaks • Breathy, hoarse quality 16 Bilateral RLN Involvement • Major concern is maintenance of airway, not phonation • Folds approximate at midline • Voice may sound normal • Abductor muscles are paralyzed, serious respiratory distress occurs • Stridor during inhalation is common • Requires tracheotomy 17 Lower Motor Neuron Disease: Bilateral muscle weakness • • • • • • • • • • Incomplete adduction of the folds Bowing of folds Inhalation stridor (as condition worsens) Hypernasality Nasal emission Reduced loudness Restricted pitch range Breathy, hoarse quality Tremor on prolonged vowels Phonemic distortions 18 LMN Disease: Respiratory Disorders • May coexist with flaccid dysphonia • Lesions of cervical, thoracic or lumbar spinal nerves may result in weakness & atrophy of speech muscles & flaccid dysarthria • Lesions may result from: trauma, tumors, & myoneural junction disease 19 LMN Disease: Respiratory Disorders • Weakness in respiratory muscles results in: -Reduced lung volume -Reduced expiratory force -Limitations in subglottic air pressure 20 LMN Disease: Voice Related Symptoms • Increased number of breaths per minute • Diminished tidal volume • Breathiness because of weak vocal fold adductors • Short breath groups • Inhalatory stridor if abductors can’t open glottis wide enough • Decreased loudness because of hypofunctional laryngeal valving • Dysphagia • Minimal intonation, stress, loudness variation 21 Management Strategies • • • • • • Postural changes and support Family counseling Physical therapy Respiratory therapy Mechanical ventilation Palatal lift prosthesis if VP inadequacy/flaccidity • Voice therapy to improve speech breathing and laryngeal adduction 22 • Alternative communication strategies Spasmodic Dysphonia • Primary Voice Symptom: Strain/Struggle • Description & Etiology: – Focal dystonia affecting laryngeal muscle control – Occurs equally in women & men – Onset in middle aged – Onset: related to URI, traumatic emotional event, begins as mild hoarseness (may be rapid or take many years – Etiologies include: Psyhcogenic, neurological (basal ganglia) 23 Spasmodic Dysphonia • Perceptual Voice Signs & Symptoms: – Adductor• • • • Struggle & strain with intermittent voice stoppage Hoarseness, harshness & tremor Creaky, tense, choked Perceptual- Strain/struggle, sudden interruption of voicing, loudness & pitch variation – Abductor• Intermittent episodes of breathy phonation • Drops in pitch & vowel prolongation's • Perceptual- Delay of voice onset following voiceless consonant 24 Spasmodic Dysphonia • Acoustic Signs: – Fundamental Frequency• Adductor (women-162 Hz; men-134Hz) • Greater variation of fundamental frequency – Vocal Intensity• Variation of amplitude • Reduced in conversation • Measurable Physiological Signs: – Airflow low & within normal limits (different studies) • Abductor-High • Adductor-Low – Pressure higher (13-14 cm H20) 25 Spasmodic Dysphonia • Observable Physiological Signs: – Laryngoscopy• Larynx appears normal • During phonation, hyperadduction(adductor), Inefficient closure (abductor), bowed vocal folds • True & ventricular fold tremor – Stroboscopy• Hard to visualize due to not being able to sustain phonation 26 Spasmodic Dysphonia • Other Considerations: – Other neurological signs• Voice tremor • Jaw • Facial jerks • Hand or limb tremor • Hyperflexia • Sucking reflex • Asymmetries in the face or palate – Possible etiologies• Brainstem abnormalities due to organic CNS disease which slows conduction within brainstem auditory pathway– Patients show abnormal ABR (capacity of brainstem to conduct impulses is impaired) 27 Spasmodic Dysphonia • Differentiating SD: – Similar features- SD, psychogenic dysphonia, musculoskeletal tension – History important & reveals differences • Psychogenic- stress, dysphonia clearly defined during stressful periods, variable (normal sometimes), respond well to voice therapy • SD- report increased stress since onset of dysphonia, minimal variability in normal productions, spasmodic not constant, do not respond well to voice therapy • Hyperfunction- consistent symptoms, do not vary phonemically, consistent vocal tension (not episodic), responds well to therapy 28 Case # 3 (CD 1; Track 3) • History: – 70 year old female – 1 year history of progressive worsening dysphonia – Intermittent periods of voice arrest & a “Squeezing” sensation during conversational speech – Active participant in a family owned business – No smoking 29 Case # 3 (CD 1; Track 3) • Examination Findings: – Oriented, no signs of language or cognitive impairment – Cranial nerve exam was unremarkable – Perceptually breathy voice quality • When asked to increase loudness- moderate-severe tremor and strain/strangled quality ensued – Acoustic Analysis• Maximum phonation time= less than 5 seconds • Fundamental frequency= 165 Hz • Jitter= 1.3% • Shimmer= 0.84 dB • Harmonic-to-noise ratio= 6.5 dB 30 Case # 3 (CD 1; Track 3) – Aerodynamic findings• • • • • • Mean airflow rate= 685 cc/sec (whispered) Mean airflow rate= 23 cc/sec (when urged to phonate) Subglottal pressure= 16 cm H20 (whispered) Subglottal pressure= 22 cm H20 (when urged to phonate) Glottal resistance= 20 cm H20 /lps (whispering) Glottal resistance= 92 cm H20 /lps (when urged to phonate) – Stroboscopic• small nodules on middle 1/3 • Persistent chink in posterior glottis • Prolonged closure time – Diagnosis: ? 31 Case # 3: Adductor Spasmodic Dysphonia with Tremor 32 Case # 3 (CD 1; Track 3) • Treatment Results– 10 sessions of voice therapy • Easy onset voice production • Increasing pitch • Humming • Sing song • Manual stabilization of the larynx • Visipitch for biofeedback • Unilateral Botox injections were recommended 33 Myasthenia Gravis • Progressive neurological disease • Manifests itself in the muscles supplied by vagus nerve • Progressive flaccid weakness or paralysis elated to muscular effort • Initially when a patient reads or speaks for a long time, gradual decrease in control of muscles of the velum and larynx • Change from normal quality to hypernasal, breathy or hoarse 34 Management of Myasthenia Gravis • Corticosteroids • anticholinesterase drugs to improve the action of the neurotransmitter chemical acetylcholine • removal of thymus gland • adrenocorticotrophic hormone therapy • palatal lift prosthesis to compensate for velar inadequacy • voice therapy to increase hyperadduction if medical treatment does not work 35 Upper Motor Neuron Disorders: Supra or Pseudobulbar Palsy • Primary Voice Symptom: – Hoarseness or harshness • Description & Etiology: – Pyramidal & extrapyramidal tracts • 2 major pathway systems that converge on lower motor neurons that control muscles of voice & speech • 1) Damage to extrapyramidal (indirect pathway) results in spasticity & increased muscle reflexes • 2) Damage to pyramidal (direct pathway) results in loss of function or skilled movements – Lesions may occur in both tracts as they are close in proximity – Effects to voluntary movement: • Spasticity, weakness, limitation of range, slowing movement 36 Pseudobulbar Palsy • Description & Etiology (cont.): – Results from progressive lesions that occur bilaterally in the corticobulbar tracts – Lesions usually result of stroke, cerebral palsy, brain injury, multiple sclerosis & arteriosclerosis – Symptoms: • Difficulty with speech & swallowing • Emotional lability • Bursts of laughter or crying 37 Pseudobulbar Palsy • Perceptual voice signs & symptoms: – Dysarthria of speech • Prosodic excess (excess rate & stress) • Prosodic insufficiency (monopitch, monoloudness, reduced stress, short phrases) • Articulatory-resonatory incompetence (imprecise consonants, distorted vowels, hypernasality) • Phonatory stenosis (harsh voice, strain/struggle, pitch breaks) 38 Pseudobulbar Palsy • Acoustic Signs: – Fundamental frequency= 124.1 Hz in men • equal or slightly higher than normal – Reduced variability of fundamental frequency – Reduced intensity variation • Measurable Physiological Signs: – Higher than normal subglottal pressure • Hypertonicity, strain/struggle – If breathy- Higher than normal airflow's – Slow opening & closing times, short closed time • inability to maintain sufficient muscle forces 39 Pseudobulbar Palsy • Observable Physiological Signs: – Laryngoscopy• No laryngeal abnormalities • Vocal fold hyperadduction may be visible – Stroboscopy• Reduced vocal fold amplitude • Diminished mucosal wave • Excessive glottal closure • Asymmetry, aperiodicity 40 Parkinson’s • Primary Voice Symptom: – Monopitch • Description & Etiology: – Progressive, degenerative disease of the central nervous system affecting basal ganglia (substantia nigra) – Decrease in dopamine in caudate nucleus & putamen • Results in rigidity, resting tremor & reduced range of movement in the limbs, neck & head • Absence of facial expression • Decreased initiating movement of command 41 Parkinson’s • Description & Etiology (cont.): – Muscles not paralyzed but hypokinetic – Respiratory movements impaired- Shallow, irregular breathing cycle – Limited vital & inspiratory capacity • Affect the ability to produce normal loudness & length speech – Causes: • • • • Unknown Linked to encephalitis lethargica Slow-growing virus Head trauma 42 Parkinson’s • Perceptual Voice Signs & Symptoms: – – – – Monopitch Excessively low pitch Harshness Variability of loudness & rate • Caused by muscle rigidity & hypokinesia • Acoustic Signs: – Fundamental frequency within the normal range • Greater variation of fundamental frequency in sustained vowels • Higher jitter values 43 • Lower SNR Parkinson’s • Measurable Physiological Signs: – Higher activity in the interarytenoid & posterior cricoarytenoid muscles – Greater activity in lip muscles • Observable Physiological Signs: – Laryngoscopy• Diminished vocal fold movement • Bowed vocal folds • Greater amplitude – Stroboscopy• Mild glottal incompetence • Tremor • Abnormal phase closure & phase symmetry 44 Case 9 (CD 1; Track 9) • History: – 72 year old male – 12 month history of progressive dysphonia – 18 months ago he was diagnosed as having Parkinson’s disease • • • • Masklike face Hand tremor Shuffling gait Stooped posture – Speech articulation was mildly imprecise • Moderate decrease of prosodic quality • Slow rate 45 Case 9 (CD 1; Track 9) • Examination Findings: – Perceptually: Moderately hoarse-breathy quality & volume was markedly reduced, pitch variations were undetectable – Maximum phonation time was WNL – Acoustic• Fundamental Frequency= 244 Hz • Jitter= .87% • Shimmer= .65 dB • Harmonic to noise= 6.9 dB – Aerodynamic• Mean airflow rate= 336 cc/sec • Subglottal pressure= 9 cm H20 • Glottal resistance= 7.6 cm H20/lps 46 Case 9 (CD 1; Track 9) – Stroboscopic• Mild atrophy of left vocal fold • Persistent glottal incompetence • Elliptical shaped chink in middle third of vocal folds • Moderate stiffness – Diagnosis: Hypokinetic dysarthria secondary to Parkinson’s • Voice therapy 2 x per week was recommended 47 Case 9: Hypokinetic Dysarthria Secondary to Parkinson’s Disease 48 Case 9 (CD 1; Track 9) • Treatment Results: – 15 voice sessions • Increasing laryngeal resistance & loudness control utilizing various vocal fold medialization techniques – Pushing on arms of chair, pulling up on bottom of chair, squeezing palms of hands together and simultaneously producing voice – Visipitch- Vocal loudness biofeedback • Isolated vowel efforts, single words, phrases, sentences & conversational speech 49 Readings • Colton & Casper: Ch. 5 • Next Directed Reading (For:10/21/99): Verdolini-Martson, K., Sandage, M., & Titze, I. (1994). Effect of Hydration Treatments on Laryngeal Nodules and Polyps and Related Voice Measures, Journal of Voice, 8, 30-47. 50