Fatima Gutierrez M.D.
Learn
when to Suspect an Immune Deficiency
Important Aspects of History Taking
Physical Exam Clues
Initial Laboratory Work-up
When to get an Immune Consult
Overview of Specialized Tests
8
or more new ear infections within one year
2
or more serious sinus infections within 1
year
Two
or more months on antibiotics with little
effect
2
or more pneumonias within 1 year
Failure
of an infant to gain weight or grow
normally
Recurrent,
deep skin or or organ abscesses
Persistent
thrush in mouth or elsewhere on
skin, after age 1
Need
2
for IV antibiotics to clear infections
or more deep-seated infections
Family
history of Primary Immunodeficiency
Sinusitis/Pneumonia
Low Antibody levels
CF
Allergic Rhinitis
Anatomy
Protein-losing
entropathy,
nephropathy
Severe eczema
Burns
2° Immunodeficiency
Malnourishment
Diabetes
Sickle Cell
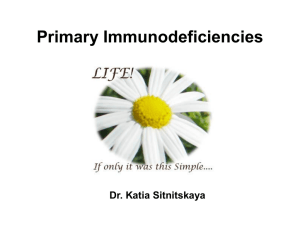
Primary
Immunodeficiencies Can Be
Categories by their Defect:
Cellular Immunity (T-Cells)
Humoral Immunity (B-Cell)
Phagocytes
Complement
Immunoglobulins
Plasma
cells
B-lymphocytes
Bone Marrow
Stem Cell
T- cells
T-Cells
directly Attack Foreign Antigens
Opportunistic
infections
Candida sp, Pneumocystis jiroveci
Persistent
Thrush
Diarrhea/Malabsorption
Poor Growth/Failure to Thrive
Unable
to make specific antibodies
Multiple / Severe Bacterial Infections
Persistent Upper Respiratory Tract Infections
Streptococcus, Haemophilis
Usually
seen after 6 months when maternal
antibodies lost
Growth usually normal unless patient with
chronic infections
Natural
Killer Cells – directly attack cells
infected with Virus
Phagocytes – ingest and kill microorganisms
Chronic Granolomatous Disease –
- Infections caused by catalase + organisms
LAD
No Pus
Gingivitis/Periodontitis
Skin Infections, Liver, GI Tract
Composed
of 30 proteins
Function in ordered integrated fashion to defend
against infection and produce inflammation
C5- C8 deficiency associated with autoimmune
C1-C4 deficiency
Associated with Rheumatic Disorders
Pyogenic Infections
C5-C9 Complement deficiency
Neiserria Infections
Basic
Screen – CH50 – measures function of
alternate pathway
Immunodeficiency
Primary
1:500 – 1:100,000 - All
1:500 IgA def
1:100,000 SCID
1:200,000 CGD
Secondary
1:300 - HIV
1:5 “unaware” of their HIV
History
Infection History
Sex
Consanguinity
History of Miscarriage/ Death in Infants
Primary Immune Deficiency in Family
History of Autoimmune/Connective Tissue d/o
Environment (Smoke, allergies)
Delayed Cord Separation (LAD)
HIV risk factors
Eczema
, Wiskott Aldrich
or Hyper IgE?
Wiskott Aldrich
Thrombocytopenia
Small platelets
Hyper
IgE -Job Syndrome
Skin infections – Staph
Sinusitis
Coarse Facies
Retain Primary Teeth
Conical Teeth
Look at Mother
Incongentia Pigmenti
Nuclear
X-Linked
Defect in Cellular Immunity
Factor – kB Essential Modulator
Variable Immunoglubulin levels
Normal B-cell numbers
Recurrent bacterial sinopulmonary and oportunistic
Infections
Ectodermal Dysplasia
Conical Teeth
Treatment Stem Cell Transplant
Lymphocyte
Absolute Lymphocyte count
Lymphopenia
Screen for B and T cell Deficiencies
Lymphocytosis
Omenn Syndrome, Leukocyte Adhesion Deficiency
Neutrophil
Count
Leukocyte Adhesion Deficiency - >100,000/mm3
Platelet
count
Size and Number
Wiskott Aldrich
WBC
total x %lymphocytes = Absolute
Lymphocyte Count (ALC)
Normal
absolute lymphocyte count 10th90th percentiles (#/μL) by age
0-3months
6-12months
1-2 years
Look
3400-7600
3900-9000
3600-8900
at normal values based on Age!!
IgG,
IgM, IgA, IgE
IgG in young infants less reliable –largely
maternal
Lab Variations! Age Adjusted Normals
Low IgG in Infant
Hypogammaglobulinemia of Infancy
Undetectable
Primary Immune Deficiency
High
IgA
Levels IgM + Absence of other Ig
Hyper IgM
IgE
Atopic Disease or Parasitic Illness, Hyper IgE
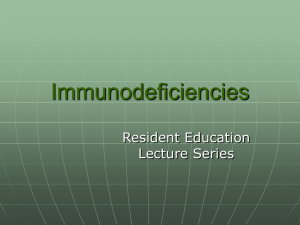
Immunoglobulin Development
•IgG nadir for infants is age 3 months to 1 year of life
•Premature infants will lack adequate maternal IgG
•Note in IgG at approximately 6 months of life (maternal vs infant sources)
•IgM production starts immediately after birth
•IgA rate of synthesis is slowest
THYMUS!
May
No Thymus
shrink in
response to
stress/surgery/infe
ction
Thymus continues
to grow until teens
Largest size
relative to body
weight at birth
T-cell
Response
Common Antigens
Candida
Trychophyton
Tetanus
Diphtheria
PPD
Anergy (no response)
Immune suppr. Meds- Steroids
Infants < 6 months / 2yrs
Malnutrition
Collagen Vascular Disease
Fever- Leukocytosis
Reaction
measured at
48 hours
HIV
– DNA when IgG unreliable
ELISA
tests IgG
Infants have Maternal IgG
Severe Hypogammaglobulinemias
Liver Disease
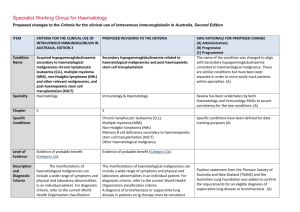
Guidelines
: www.aidsinfo.nih.gov
Measurement of
Specific T, B, NK
and phagocytic
cells
The Case of SCID
NK Cells
TcellsB-Cells
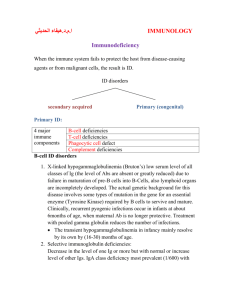
Tests your Body’s Ability to
Make Antibodies – Majority
of Vaccines activate Bcells in the presence of Tcell
Tests for Common Vaccines
Diphtheria
Tetanus
Streptococcus
Normal Response
Diphtheria > 0.1
Tetanus > 0.1
Or…
4 fold increase of baseline 1
month after vaccine given
Streptococcus – Note minimal
response
Serotypes in Prevnar:
4, 6B, 9V, 14, 18C, 19F, 23F
Serotypes in PCV13
Serotypes 1, 3, 4, 5,
6A, 6B, 7F, 9V, 14,
18C, 19A, 19F, 23F
Measures the ability of
lymphocytes to respond to
mitogens and Specific
antigens
Strongly Mitogenic on T-Cells
- PHA (Phytohemagluttin)
- ConA (Concanavalin-A)
Minimal Response
Assay working well
Stimulates T&B cells (Mitogen
- Pokeweed
Antigens:
- Candida
-Tetanus
- Dipthera
*Prior exposure required for
response !! > 2yrs age
Early
Recognition of Primary Immune
Deficiency – Many Primary Immune
Deficiencies are Lethal!
Recognize
Don’t
Lab Value Diversity
forget to look for HIV
Noroski MD, L., Shearer MD, W. Short Screening for
Primary Immunodeficiencies in the Clinical
Immunology Laboratory. Clinical Immunology and
Immunopathology. Vol. 86, No3, March pp. 2237-245,
1998
Fleisher, Shearer, Kotzin, Schroder. Clinical
Immunology – Principles and Practice 2nd Ed. Rich, R.
Schmitz PhD, Folds PhD. Clinical and Laboratory
Assesment of Immunity. Journal of Allergy and
Immunology 2003: 111:S702-11
American Academy of Allergy Asthma and Immunology
– www. aaai.org
Immune Deficiency Foundation – primaryimmune.org
Jeffrey Modell Foundation www. jfmworld.org