IU Health and the Transformation of U.S. Health Care
advertisement

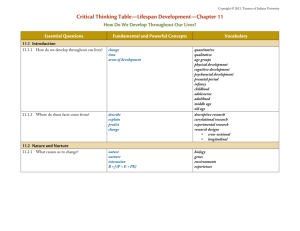
The Structure of Academic Health Systems and the Origins of IU Health Prepared for: American Dental Education Association 54th Annual Deans Conference Daniel F. Evans, Jr. President and Chief Executive Officer November 11, 2012 4/8/2015 1 Structure and Organization of Academic Health Systems • Academic health systems – a combination of a medical school and an owned or affiliated health care system (can also include other health professional schools) • Two primary organizational models 1. Fully integrated model – education, research, and clinical functions report thru university leadership and university board of trustees 2. Split model – education and research functions report thru university but clinical functions ( the health system) report thru an affiliated but separate and independent leadership structure and board • University of Michigan is an example of first model. CEO of UM health system is also the EVP for Medical Affairs at the University • IU Health is an example of the second model. The Dean of the Medical School and the health system CEO are two different people and report to separate Boards Academic Health System: Benefits of Alignment Increased patient referrals, clinical faculty, improved outcomes & overall success of clinical enterprise. Investment of clinical practice & health system income in academic enterprise Improved structure & visibility for clinical & research enterprises & for the academic health system as a whole. Increased research productivity, technology transfer, leverage to external support. IU Health – Governance Structure Methodist Health Group, Inc Board of Trustees (Methodist Class) Indiana University Board of Trustees (University Class) Indiana University Health Board of Directors Indiana University Health IU Health is sole “corporate member” of affiliated hospitals and appoints majority of their boards IUHP Board Of Directors (Includes 2 reps from IU School of Medicine) Indiana not-for-profit 501 (c)(3) IU Health Hospitals (18 statewide) IU Health Physicians (IUHP) History of IU Health • In 1997, Methodist Hospital of Indianapolis merged with two hospitals owned by Indiana University – IU Hospital and Riley Hospital for Children – to form Clarian Health • The merger was a response to existing and anticipated changes in the health policy environment: – – – – reductions in state funding for IUSM impact of managed care need for larger referral base for IU Hospital desire to increase market leverage and achieve efficiencies by combining resources – important for IUSM to expand surplus from clinical services to support education and research missions • A similar rationale has been used for other mergers and alliances between health systems and medical schools that occurred at this time and since History of IU Health (cont) • Clarian changed its name to IU Health in 2011 to better reflect the close relationship between the health system and the School of Medicine • Indiana University Health has grown substantially since the formation of Clarian Health in 1997 – it is now largest health care system in Indiana and a top 10 academic health system in the U.S. – – – – 18 hospitals state-wide $5B in annual revenues More than 1,000 employed physicians IUH Methodist is largest tertiary/quaternary hospital in IN. More than 30% of patients uninsured or on Medicaid – IUH Riley Hospital for Children is state’s only comprehensive children’s hospital Challenges Facing Academic Health Systems • Health Care Reform (the Affordable Care Act) • Pricing Pressures Across Payer Classes – Medicare and Medicaid affected by federal and state budget challenges – Employers struggling to afford premiums and passing more costs onto employees. Impact of new health insurance exchanges in 2014? – Payers showing greater willingness to exclude expensive providers, even of high quality (narrow networks”) • Shifting Payer Mix as Baby Boomers Retire and get Medicare • Mantra among health system executives: “manage to Medicare margins” = 20-25% reduction in cost structures • Big challenge for academic systems given education and research commitments and costs The Transition to Accountable Care • The term “accountable care” refers to health care delivery and payment models in which providers assume some level of financial risk for the clinical and financial outcomes of the care they provide to a defined population of patients. Key Concepts of Accountable Care • Keep patient well vs. treat patient when sick • Emphasis on primary and preventive care – Importance of oral health and hygiene • Care management and coordination critical • Use of evidence-based practice to reduce unnecessary clinical variation and improve quality of outcomes • Manage utilization to control total cost of care per person • Providers rewarded for quality and efficiency, not volume of care provided • Expanded information technology; robust decision support tools