923-Bbosa-_b
advertisement

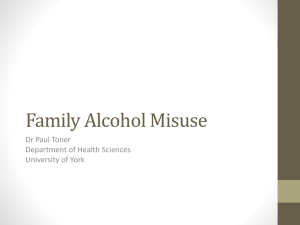
923 Effect of Interventions on Misuse of Antibiotics/Antibacterial Drugs in Developing Countries: a Systematic Review Bbosa, Godfrey Sande1,2; Wong, Geoff2; Kyegombe, David B3; Ogwal-Okeng, Jasper1 1: Makerere University College of Health Sciences, Uganda 2: University of London, United Kingdom 3: Kampala International University Medical School, Ishaka Campus, Uganda 1 2 Introduction • Misuse of antibiotics/antibacterial drugs is a global problem especially in developing countries with poor healthcare systems & corruption • Occurs at all levels in both public & Private Healthcare facilities • Reported up to 75 % of antibiotics are prescribed inappropriately in teaching hospitals in developing countries (Nambiar, 2003) • Are used in conditons where not needed like flu etc. • Resulted in failure of eradicating infectious bacteria, emergence of resistance, waste of resources, increased cost of treatment, ADR & death (Kardas et al., 2005) 3 Many Factors Influence Use of Medicines Policy, Legal and Regulatory framework Prescriber, Dispenser & their workplaces Rational Drug Use Patient & community Drug Supply System Interventions are directed at these components 4 5 Objectives of the review • Review determined effect of various intervention studies on AB misuse in developing countries Research question 1. What are the various interventions measures used in controlling irrational use of antibiotics/antibacterial agents in developing / poorer nations? 2. What is the impact of various intervention measures used in controlling the irrational use of antibiotics/antibacterial agents in developing / poorer nations? 6 Methods • Study design: A systematic review • Search strategy: was developed to retrieve relevant articles from various databases including: – Medline/PubMed – Embase – INRUD/Management Sciences for Health (MSH) – WHO – Cochrane – Google scholar search engine was used to retrieve more studies from Journal articles & abstracts – Gray literature by manual method 7 Criteria for inclusion and exclusion of studies in the review • All the studies included in the review followed PICO-DTS where: – Patient, population, or problem (P) – Intervention, independent variable, or exposure (I) – Comparators (control) (C) – Dependent variables or outcomes of interest (O) – Study design (D) – Timing (T) – Study setting (S) (Moher & Tricco, 2008; Stone, 2002) • All studies were included or excluded basing on each of the above 8 Data extraction & storage of primary data • Data was extracted using the designed data extraction sheet basing on aims of review criteria: – Geographical location of where study was conducted based (World Bank Country Classification, 2010). – Categories & subcategories of intervention - Education - Managerial - Regulatory - Diagnostic - Managerial/education - Economic/financial - Education/regulation - Multifaceted (Combination of almost all) – Study settings - Hospitals - Public Healthcare facilities - Community - Out-patients Departments - Private Pharmacies/ drug stores – Outcome measure basing on effect & effect size on AB 9 10 Quality of evidence • Quality was judged by Appraisal of individual primary research studies for inclusion in reviews (Gough, 2007): A = Trustworthiness of results (Methodological quality) B = Appropriateness of use of that study design for review's research question (Methodological relevance) C = Appropriateness of focus of research for answering the review question (Topic relevance) D = Judgment of overall weight of evidence (WoE) based on assessments made for each of criteria A-C • Each of the studies were assessed as follows: 1-Strongly Agree 5- Agree 10 –Disagree or using Yes (Y) or No (N) or Not applicable (NA) 11 Results Articles retrieved and screened 12 13 14 15 16 17 18 19 Discussion • A total of 722 articles were retrieved and 55 were reviewed – 10.9% were from Africa, 63.6% from Asia, 9.1% from Latin America & 16.4% from South-eastern Europe • A total of 52.7% were hospital settings, 5.5% outpatient departments, 21.8 public health care facilities, 12.7% private pharmacies/drug stores, and 7.3% communities • Education intervention was 27.3% – With group discussion having 19.2% mean reduction in AB use, 27.6% in AB prescription & 41% belief of no AB use – Community training had 30.5% reduction in AB use (highest), 23.8% mean reduction in AB prescription & 36% belief of no AB use 20 • Managerial was 20% with 8% improvement in AB dose – 8–100% AB use adherence & 31.8% mean reduction of AB receipt – 29.1% change of AB in resistance cases and 9.8-100% reduction in prophylactic AB use. • Managerial/education was 3.6% with 4.7% reduction in AB prescription • Regulatory was 9.1% with 60.5% improvement in AB use in restriction unlike 16.4% in non-restriction • Education/regulation were 9.1% – with 8% reduction in non-indicated AB, 24% improved AB use rate, 14% mean appropriate AB use improvement – 11.1% reduction of incidence of bacterial resistance – 75.1% reduction in AB use in diarrhea, 42.4% reduction in scabies, 13.8–33.6% reduction in AB use in ARI – Overall 60% reduction in AB use 21 • Diagnostic was 3.6%, with 68% reduction in AB use after diagnostic test as compared to100% in control – Was 73% likelihood of AB use in +test vs 87% in –ve test • Multifaceted interventions were 27.3% – 63% improvement in appropriate AB doses prescribed (best), 2.6 mean no. of AB encounter reduction, 23% AB prescription reduction – 18.3% generic AB prescribing improvement, 32.1% reduction in AB use, 89% reduction in AB use in ARI, 82% in surgery, 62.7% mean reduction in deliveries, 39% in STDs, 36.3% mean reduction in diarrhea, 14.6% mean reduction in malaria – 6–11% reduction cost of treating bacteria-resistant organisms – Some studies, was 6.3 reductions in mean AB encounters after 1 month of intervention, then increased to 7.7 after 3 months hence lack of sustainability of intervention programme as observed in some studies • No study on economic/financial intervention found 22 Conclusion • Misuse of antibacterial/antibacterial drugs is on increase especially in developing countries • Variety of interventions are used for irrational use of AB drugs & had some impact • Most of interventions were done in Asia • Multifaceted interventions are effective in reducing misuse & inappropriate use of AB drugs & reduce emergence of resistance to commonest bacteria in developing countries • Some studies showed a tendency of reverting once intervention programme stops 23 Acknowledgments & Source of funding • Acknowledge staff of Common Wealth Scholarship programme & staffs of University of London, Department of Primary Care & Population Health (PCPH) for their support especially Prof. Petra Boyton, Prof. Ceri Butler, Prof. Trish Greenhalgh & others • Funding Source: – Common Wealth Scholarship Programme and University College London, Department of Primary Care and Population Health (PCPH) 24 End