Dr Megan Rowley - diamondblackfan.org.uk
advertisement

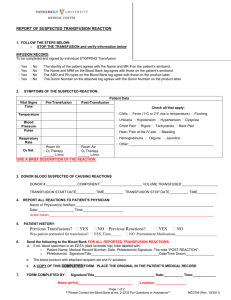
+ Blood Transfusion Dr. Megan Rowley Consultant in Transfusion Medicine + What would you like to know? Where does my blood come from? What happens to blood once it has been collected? What is in a bag of blood? Is blood safe and what happens if it goes wrong? How do you decide when to transfuse? And how much? Who are all the people who make this work? + There are lots of people who work hard to get blood to you Blood donor and the blood collection teams NHS Blood and Transplant Hospital Transfusion Department Doctors and nurses who look after you EXPERTS PEOPLE WHO ADVISE ON BEST PRACTICE REGULATORS PEOPLE WHO OVERSEE ADVERSE EVENTS + Healthy Blood donors aged 17-65 can donate every 4 months Fill out a donor health questionnaire and have a haemoglobin check Fixed and mobile donor sessions – a masterpiece of organisation! Where does my blood come from? www.blood.co.uk Look on the website – lots of interesting facts, figures and video clips + What happens to blood once it has been collected? 1. Tested Blood group ABO D positive or negative Other blood group antigens Viruses and other infections Hepatitis B and C HIV 1 and 2 and HTLV1 Syphilis (Malaria) (Cytomegalovirus) + What happens to blood once it has been collected? 2. Processed No such thing as ‘whole blood’ What we need are ‘components’ RED CELLS PLATELETS PLASMA And the white cells have to be removed LEUCODEPLETION + What is in a bag of blood? Red Cells in Optimal Additive Solution (SAG-M) Shelf-life 35 days at 4°C No white cells or platelets and very little plasma UK Blood Donors Distribution of blood groups varies across the world Blood Group RhD Positive RhD Negative Total O A B AB 37% 35% 8% 3% 7% 7% 2% 1% 44% 42% 10% 4% How do we choose which blood group to give? DONOR BLOOD GROUP PATIENT BLOOD GROUP + ANTIBODI ES IN THE PATIENT O A B AB O Anti-A and AntiB GOOD BAD BAD BAD A Anti-B GOOD GOOD BAD BAD B Anti-A GOOD BAD GOOD BAD AB None GOOD GOOD GOOD GOOD + Matching blood Before transfusion of red cells the blood has to be appropriately matched to the patient The transfusion lab will select the correct ABO/D red cell group for the patient Some patients also have ‘special requirements’ e.g. IRRADIATED, KELL NEG Serological (XM) is where the patient’s plasma is mixed with the donor’s red cells Takes 40 minutes Electronic Issue (EI) is where the computer checks there are two patient blood groups that agree, there is a is valid (recent) G&S sample and a negative antibody screen Takes 10 minutes Labelling and Issue A blood bag with a compatibility label attached All the information on the blood bag label is bar-coded as well as eye readable + Is blood safe? Yes! Most of the time…. If blood transfusion is the only treatment for your condition and the consequences of not having a blood transfusion outweigh the the risks of having one then it is then having a blood transfusion is the right thing to do Patient blood management + Patient Blood Management Patient information and valid consent Give the right amount of blood Consider and discuss alternatives Consider special requirements Minimise anaemia Review the outcome + Patient Information and Consent ‘Valid’ consent is required for transfusion (verbal) Alternatives should be offered if appropriate If transfused in an emergency, patient must be informed afterwards Involve patients in the process to ensure they get the right blood and the right ‘special requirements’ + Why and when do we give blood? The decision to transfuse is based on the whole clinical picture Is the patient bleeding? What are the blood results? Is the patient symptomatic? Will a transfusion solve the problem? What are the risks of transfusion? Are there alternative treatments? 4mL/kg will typically give a Hb increment of 10g/L = 1unit RBC gives a Hb increment of 10g/L in a 70-80 kg patient ‘The decision to transfuse must be based on a thorough clinical assessment of the patient and their individual needs. The rationale for the decision to transfuse and the specific components to be transfused should be documented in the patients’ clinical records’ BCSH guidelines 2012 + What happens if it goes wrong? Investigate incidents locally Report serious hazards via a national system SHOT Clinical audit ROOT CAUSE ANALYSIS PROCESS and APPROPRIATNESS of TRANSFUSION Learn and continuously improve DOCTORS and NURSES TRANSFUSION LABORATORIES BLOOD SERVICES EXPERTS and REGULATORS + What reactions occur with red cells? + Serious Hazards of Transfusion 1996-2012 (n=11570) Getting an infection from blood Getting too much blood too quickly Having a reaction to blood Getting the wrong blood + Adverse effects of RBC transfusion contrasted with other risks Hepatitis and HIV transmitted by transfusion is very rare Carson J L et al. Ann Intern Med doi:10.1059/0003-4819156-12-201206190-00429 ©2012 by American College of Physicians Fluid overload from blood transfusion and patients with a fever during transfusion is quite common + Conclusion Blood is a precious gift given by a blood donor There are many people working behind the scenes to get you the right blood at the right time, every time Each bag costs £120 but all of that goes towards collecting blood making it safe and getting it to the hospital – no money goes to the donor If it goes wrong we do our best to understand why and continually improve It is important that you understand the risks and benefits of transfusion and give your consent to receive this treatment The team caring for you need to tailor your blood support to you personally and to check it is having the desired effect