Dia 1 - Progetto LIBRA
advertisement

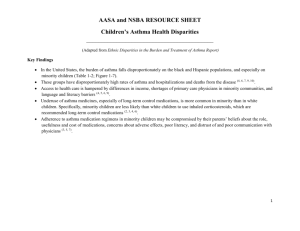
Grazie per aver scelto di utilizzare a scopo didattico questo materiale delle Guidelines 2011 libra. Le ricordiamo che questo materiale è di proprietà dell’autore e fornito come supporto didattico per uso personale. Phenotyping severe asthma The U-BIOPRED project p.j.sterk@amc.nl Department of Respiratory Medicine Academic Medical Center University of Amsterdam The Netherlands Towards phenotyping severe asthma 1. What is a phenotype? 2. What is the concept behind unbiased disease-fingerprinting? 3. Is this needed for the management of severe asthma? 4. The IMI-EU project U-BIOPRED 5. The promiss of ‘systems medicine’ What is a phenotype? The composite of observable characteristics of an organism… resulting from interaction between its genetic make-up and environmental influences… that is relatively stable, but not invariable with time. The three determinants of a phenotype Genetics Time Environment Complex biological systems: The secret of life • Spontaneous self-organisation • Open systems, importing energy, exporting waste • Not linear: output not simply proportional to input • Sudden emergent phenomena, deterministic chaos • Adaptation by negative feedback loops • Fluctuating: homeokinesis rather than homeostasis Schrödinger E. Lectures Trinity College Dublin; 1944. New York: MacMillan Goldberger AL. Proc Am Thoracic Soc 2006;3:467-472. Macklem PT. J Appl Physiol 2008;104:1844-1846. Macklem PT & Seely A. Perspectives Biol Med 2010;53:330-343. Genes, environment and time Richards K. Life. Little, Brown & Company, London, 2010 Genes Cell differentiation & activation Gene-& posttranscriptional regulation Organ structure & function Cell-cell interaction Organism health & disease Macro physiology Capturing phenotypes disease domain diagnosis & therapy Symptoms √ Functional √ Cellular ? Molecular ? Severe asthma Facts – Despite all our attempts, the clinical course of severe asthma is far from optimal – Unfortunately, the development of new drugs for severe asthma has not been successful during the past years Reasons? – Severe asthma is not a single disease: individual patients are clinically very different – There are multiple and co-existent disease mechanisms – At present the efficacy of new drugs cannot be predicted well enough from preclinical models nor from currently defined patient characteristics Asthma severity and control No treatment controlled mildest Intensive treatment mild mild severe severe uncontrolled most severe Cockcroft & Swystun JACI 1996;98:1016-1018 ATS/ESR Task Force Asthma Control and Exacerbations Taylor et al. ERJ 2008;32:545-554 Reddel et al. AJRCCM 2009;180;58-99 “Severe asthma” Problematic asthma Fixed obstruction Uncontrolled asthma Non-adherent asthma Exacerbation prone Co-morbid asthma Refractory asthma Truly severe asthma Difficult asthma no asthma NAEPP 1997, ERS 1999, GINA 2002, ATS & SARP 2002, ENFUMOSA 2003, BIOAIR 2005 TENOR 2004, Paris 2007, ERS 2008, PSACI 2008, WHO 2009, U-BIOPRED 2011 Consensus Definition and classification 1. Problematic asthma • 2. All asthma that remains uncontrolled despite prescription of high intensity treatment Difficult asthma • • • • 3. Mild-moderate asthma that remains uncontrolled Adherence <50%, VCD, dysfunctional breathing, psychosocial Persistent exposures Untreated co-morbidity Severe asthma • • • • Poor control or >2 exacerbations/year, despite high intensity treatment > 1000 (adults) or 500 (children) μg FP equivivalent or daily oral steroids, combined with LABA or other add-on medication Mainted control only achievable by high intensity treatment Thereby serious risk of adverse effects Bel et al. U-BIOPRED Study. Thorax 2011 EPub SARP Severe Asthma Cluster Analysis Early onset Atopic Normal pb FEV1 < 2 Controllers 1 Early onset Atopic Normal pb FEV1 More medications 2 Late onset Older Obese Female Lower pb FEV1 Exacerbations 3 Long duration Very low FEV1 Reversibility Long duration More women Less atopic Very low FEV1 Not reversible 4 Moore et al. Am J Respir Crit Care Med 2010;181:315-323 5 Asthma: complex biology Normal asthma Central Peripheral Mauad, Bel, Sterk. J Allergy Clin Immunol 2007;120:997-1009 Additional phenotypic markers? When will a disease marker be useful? ● ●● ● ● ● ● ● ● Reference feature Marker B Marker A ● ● ● ● ● ● ● ● ● ● ● ● Reference feature Disease markers which provide complementary information in asthma Factor analysis Age FEV1 FVC PC20 Reversibility Sputum - eosinophils - ECP Rosi et al. JACI 1999;103:232 Phenotypic cluster analysis in asthma Symptoms Discordant Symptoms Obese Late onset Controlled Mixed onset Discordant Inflammation Eosinophilic inflammation Haldar et al. Am J Respir Crit Care Med 2008;178:218-224 Exhaled nitric oxide + FEV1 predict lung function decline in severe asthmatics during 5 years prospective follow-up Baseline FEV1 ≤ 80% 200 100 Change in FEV1 (ml) Change in FEV1 (ml) Baseline FEV1 > 80% 50 0 -50 -100 -150 150 100 50 0 -50 -100 -200 1 2 4 8 16 32 64 128 1 Exhaled NO (ppb) Van Veen et al, ERJ 2008;32:344-349 2 4 8 16 32 64 Exhaled NO (ppb) 128 Heatmap for molecular phenotyping from cytokines in BAL of severe asthma Brasier et al. J Allergy Clin Immunol 2008;121:30-37 Transcriptomic phenotypes from sputum in asthma Baines et al. J Allergy Clin Immunol 2011;127:153-160 Protein expression profiling in serum in asthma, COPD, cystic fibrosis and controls (SELDI-TOF-MS signatures) Asthma vs COPD Asthma vs CF COPD vs CF AUC of ROC 100% 100% 100% Gomes-Alves et al. Clin Biochemistry 2010;43:168-177 Electronic nose analysis Fens et al. Am J Respir Crit Care Med 2009:180:1076-82 Training and validation sets by eNose: asthma versus COPD Accuracy: 85% AUC: 0.93 ●Training set COPD ●Training set asthma ▄Validation set COPD ▄Validation set fixed asthma Fens et al. ATS 2010, submitted disease domain diagnosis & therapy Symptoms √ Functional √ Cellular ! Molecular ! disease phenotype Continuous recording and fluctuations of respiratory resistance in asthma Rrs at 10 Hz (cmH2O/l/s) mild Asthma subject 2 5.5 5.0 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0 20 40 60 80 100 120 time Slats et al. Am J Respir Crit Care Med 2007;176:121-128 Respiratory impedance in asthma and COPD Asthma COPD Muskulus et al. J Appl Physiol 2010;109:1582-1591 Multi-dimensional, non-parametric fluctuation analysis of the dynamics of respiratory impedance in asthma and COPD Muskulus et al. J Appl Physiol 2010;109:1582-1591 Discriminant score ROC curve using 5-dimensional reconstruction of respiratory impedance dynamics in discriminating asthma and COPD Asthma Muskulus et al. J Appl Physiol 2010;109:1582-1591 COPD disease domain diagnosis & therapy Symptoms √ Functional √ Cellular ! Molecular ! disease phenotype University of Amsterdam University of Southampton Imperial College London University of Manchester University of Nottingham Fraunhofer institute Hannover Centr Nat Recherche Sc Villejuif Paris Université de Méditerranee Montpellier Karolinska Institute Stockholm University Umea UniversityTor Vergata Rome Università Cattolica del Sacro Cuore Rome University of Catania Hvidore Hospital Copenhagen University Hospital Copenhagen Haukeland University Bergen Semmelweis University Budapest Jagiellonan University Krakow University Hospital Bern University of Ghent Novartis GlaxoSmithKline AstraZeneca Chiesi Pfizer Roche UCB Boehringer Ingelheim Johnson & Johnson Almirall Netherlands Asthma Foundation Asthma UK European Lung Foundation EFA Int Primary Care Respir Group Lega Italiano Anti Fumo Biosci Aerocrine Synairgen Philips Research Hypothesis U-BIOPRED study Biomarker profiles from multi-scale molecular, physiological, and clinical data integrated by an innovative systems biology approach into distinct handprints will enable the prediction of clinical course and therapeutic efficacy and identification of novel targets in the treatment of severe asthma www.ubiopred.eu 1025 subjects including adults ánd children Adults Children Severe asthma 525 100 Mild asthma 100 50 Healthy controls 100 Infants severe recurrent wheeze 100 Infants mild recurrent wheeze 50 Study design 1. Severe asthma consensus and diagnostic algorithm (Bel et al. Thorax 2011 EPub) 2. Cross-sectional comparitive handprint discovery 3. Longitudinal follow-up during 30 months 4. Iterative comparison handprints from preclinical models (human ex-vivo, animal in vivo) 5. Proof of concept intervention by randomized controlled trial www.ubiopred.eu Study design exacerbations tele-monitoring bronchoscopy screening baseline follow-up 1 -1 0 3-6 Months Follow-up 2 24-30 U-BIOPRED Workpackages 1 Coördination and management Sterk, Higenbottam, Wagers, Sondervan 2 Consensus generation Bel, Compton 3 Cross-sectional and longitudinal cohorts Chung, Gerhardsson 4 Bronchoscopic assessment Chanez, Sousa 5 Pre-clinical human models Krug, Lewis 6 Pre-clinical laboratory models Adcock, Knowles 7 Omics technologies Djukanovic, Corfield 8 Bioinformatics and systems biology Auffray, Manta 9 Dissemination Wagers, Compton 10 Ethics De Boer, Higenbottam ‘Systems Medicine’ Patient reported Clinical Functional Cellular Molecular Auffray, Adcock, Chung, Djukanovic, Pison, Sterk. Chest 2010;137:1410-1416. www.ubiopred.eu Ensure quality Genomics Transcriptomics Proteomics Metabolomics Cytology Histology biobanking Unresolved disease problem Quantitative morphology (imaging) Integrate data Formalize questions Organ function and dynamics Clinical expression and patient perception knowledge repository Perturb the system Refine unbiased computational model by iteration Generate hypotheses Add open source public data Kaminsky, Irvin, Sterk. J Appl Physiol 2011: EPub. Kaminsky, Irvin, Sterk. J Appl Physiol 2011, EPub. Conclusions • Phenotypes are integral descriptions of biological systems from the molecular to organism level • They are not stable, being modulated by genes, time and environment • In asthma and COPD there is increasing evidence that multi-dimensional biomarker signals are complementary to clinical characteristics • Unbiased cluster- and time-series analysis by using a systems medicine approach can make a step-change from traditional diagnoses to “phenotype-handprints” • U-BIOPRED is validating this strategy for severe asthma p.j.sterk@amc.nl