Neonatal Sepsis - Colorado Perinatal Care Council

• Differentiate between the evaluation of a symptomatic newborn and the assessment of risk factors in an asymptomatic infant at risk for sepsis
• Review obstetric risk factors for neonatal sepsis in an asymptomatic newborn
• Review diagnostic tools for evaluation of sepsis in an asymptomatic newborn
• Symptomatic infants require prompt diagnostic testing and institution of antibiotic therapy given the rapidity of deterioration and the high likelihood of successful treatment in infants with true bacteremia.
• The need for clinical judgment in this decision-making process precludes the use of an algorithm or protocol.
• Respiratory distress/grunting
• Lethargy
• Irritability
• Hypothermia
• Hypoglycemia
• Hypotonia
• Acidosis
• Apnea
• Cyanotic spells
• Poor perfusion
• CBC with manual differential-WBC corrected for NRBCs
• Blood culture
• A significant number of infants with meningitis will have a negative blood culture. A lumbar puncture may be considered if:
– the infant has specific symptoms of meningitis
– symptoms more suggestive of sepsis than MAS or RDS
– the blood culture is positive
• Urine culture is not indicated
• Tracheal aspirate/gastric cultures may be useful in the first 12 hours of life. A positive culture may be found in
44% of infants with clinical pneumonia and a negative blood culture.
Gram positive, beta hemolytic bacteria
Common colonizer of human gastrointestinal and genitourinary tracts
Recognized as causing disease in humans in the
1930s
Causes serious disease in young infants, pregnant women and older adults
Emerged as most common cause of sepsis and meningitis in infants <3 months in the 1970s
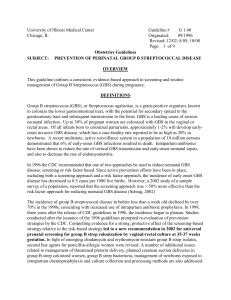
Early-onset: 0-6 days of life
90
80
70
60
50
40
30
20
10
0
Late onset: 7-89 days of life
< 1 wk
1-3 wk
1 2 3 4 5 6 7 8 9 10 11
Age (months)
A Schuchat. Clin Micro Rev 1998;11:497-513.
50%
Non-colonized newborn
GBS colonized mother
50%
Colonized newborn
98%
Asymptomatic
2%
Early-onset sepsis, pneumonia, meningitis
Early-onset GBS
Late-onset GBS
Before national prevention policy Transition Universal screening
Source: Active Bacterial Core surveillance / Emerging Infections Program
• Penicillin the first-line agent for IAP
• Dosage: 5 million IU IV then 2.5-3.0 million IU IV every 4 hours
• Revised dose (2.5-3.0 million IU) consistent with available penicillin formulations
• Ampicillin an acceptable alternative
Antibiotics for IAP in Women Allergic to Penicillin
• Cefazolin best option for a woman allergic to penicillin but not at high risk for anaphylaxis
• Drugs with less evidence for effectiveness (e.g. clindamycin, vancomycin) only for women at high risk of anaphylaxis
– High risk for anaphylaxis defined as history of anaphylaxis, angioedema, respiratory distress or urticaria following penicillin
• Erythromycin no longer included as option
• On the basis of signs and symptoms:
– fever (which might be low-grade)
– uterine tenderness
– fetal tachycardia
– maternal tachycardia
– foul-smelling or purulent amniotic fluid
• Fever alone in labor may be used as a sign of chorioamnionitis and hence indication for antibiotic treatment
• In Manroe ’ s 1977 study all 45 infants had clinical signs of sepsis by 14 hours
• Time to onset of symptoms is not delayed by maternal antibiotics: CDC surveillance (GBS)
– 208 no abx 60 min prior to delivery; median illness 2 hours of life range 0-144 hours
– 33 got abx > 60 min prior to delivery; median illness 0 hours of life range 0-19
• PROM >18 hours 1%
• Maternal + GBS (preprophylaxis era)
• Maternal + GBS (in prophylaxis era)
• +GBS and chorioamnionitis
0.5-1%
0.2-0.4%
• Maternal + GBS + PROM, fever or preterm 4-7%
• Chorioamnionitis 3-8%*
6-20%
• PROM + preterm
• PROM + low Apgar score
4-6%
3-4%
• Prematurity. The risk of sepsis from any cause starts and continues to rise at any gestation < 36 weeks.
*Escobar, Pediatrics, 2000
• N=12
• 25% would start antibiotics for asymptomatic chorioamnionitis without other evidence
• 75% wanted screening tests first
Adjunctive test
ANC <= 1750
I/T >= 0.2
I/T >= 0.25
I/T >= 0.3
Sensitivity (%)
38-96
90-100
45
35
CRP > 1.0 mg/dL 70-93
*WBC <= 5000
I/T >= 0.2
CRP > 1.0 mg/dL
* 2/3 tests positive
100
PPV (%)
20-77
11-51
6
7
7-43
27
NPV (%)
96-99
99-100
98
98
97-99.5
100
• Two CRP levels <1 mg/dL obtained 24 hours apart, 8 to 48 hours after presentation, indicate that bacterial infection is unlikely.
• The sensitivity of a normal CRP at the initial evaluation is not sufficient to justify withholding antibiotic therapy.
• CRP elevation begins 4-6 hours after the onset of sepsis (or other stimulus) and peaks at 24-48 hours.
• The positive predictive value of elevated CRP levels is low.
• Fastidious organisms, maternal antibiotic treatment and small volumes
(<1ml) decrease sensitivity
• Contamination with skin organisms
• Molecular methods may eventually improve detection in less time
• Purpose was to differentiate “ wet lung ” from GBS pneumonia
• No sensitivities or predictive values were calculated
• Upper limits of normal for I:T ratios were
“ designated ”
• Combine sensitivity and specificity
•
(probability that person with disease has positive test) sensitivity
(probability that person without disease has positive test) 1-specificity
• A person with disease A is “___” more times likely to have a positive test than someone without the disease
• “Pre-test probability” is estimated based on personal experience, prevalence data, published reports, etc.
• The test is used to modify pre-test probability to “post-test probability”
• Post-test odds = pre-test odds x LR
• 34 weeks and up, 350 cases (cultureconfirmed bacterial sepsis at <72 hours) from 608,014 births
• Combining cutoff methods (ROM>x,
T>x, GA<x) flags 17% of population at risk but only identifies 47% of sepsis cases
VARIABLE
37-40wk
34-36wk
41wk-
ROM < 12hr
12-17.9 hr
18-23.9 hr
24 hr-
<100.5
100.5-101.4
101.5-102.4
102.5-
OR ref
2.56
1.62
ref
3.65
VARIABLE
GBS -
GBS +
GBS -/UNK
GBS +
No intrapartum abx
2.81
14.8
ref
4.53
Any antibiotic
GBS IAP
Broad spectrum abx
Abx < 4 hr prior to del
1.91
1.77
6.25
ref
20.08
Abx > 4 hr prior to del .34
103.
37
OR
REF
1.14
REF
1.38
Ref
• 67,623 34 week and up infants, 245 positive blood cultures
• GBS 56%(decreasing over time)
• Ecoli 22%
• Enterococcus 4%
• Other 18%
Test
WBC x 10 3 /ul
0.4.99
5-9.99
10-14.99
15-19.99
20-
ANC x 10 3 /ul
0-0.99
1-1.99
2-4.99
5-9.99
10-
I/T
0-0.14
0.15-0.29
0.3-0.449
0.45-0.599
0.6-
1.3
1.4
4.8
6.1
1.2
LR
7.5
2.3
1
0.89
0.93
LR
0.45
<1 hour
LR n/a
1.4
1.1
0.73
1.2
2.9
3.3
8.4
0.77
LR
33.5
9.3
1.1
0.92
0.55
LR
0.46
1-3.99 hours
LR
27.6
2.4
0.65
0.64
0.16
LR
115
51.7
6.9
0.64
0.31
LR
0.25
4+ hours
LR
80.5
6.4
1.0
0.41
1.2
3.1
8.8
10.7
• 38 week infant, asymptomatic, mother diagnosed with chorioamnionitis
• Temp 101.5, GBS+ antibiotics >4 hours prior, ampicillin. ROM 28 hours
• What is pretest risk based on experience?
• Based on Escobar’s paper? (0.23%)
• CBC WBC count 22.5K (LR1.2, .77, .06)
• I/T ratio of 0.3 (LR 1.4, 2.9, 3.1)
• ANC 6000 (LR .89, .82, .64)
• 38 week infant, asymptomatic, mother diagnosed with chorioamnionitis
• Temp 103, GBS+ antibiotics >4 hours prior, ampicillin. ROM 24 hours
• What is pretest risk based on experience?
• Based on Escobar’s paper? (2.21%)
• CBC WBC count 4K (N/A, 27, 80)
• I/T ratio of .6 (LR 6, 8.4, 10.7)
• ANC 750 (LR 7.5, 33.5, 115)
• 40 week infant, asymptomatic, mother diagnosed with chorioamnionitis (no question)
• No prenatal information
• What is pretest risk based on experience? (5%?)
• CBC WBC count 4K (N/A, 27, 80)
• I/T ratio of .6 (LR 6, 8.4, 10.7)
• ANC 750 (LR 7.5, 33.5, 115)
I/T ratio .3
I/T ratio .6
ANC < 1000
I/T ratio .3
I/T ratio .6
ANC < 1000