Change Management from *Home visit* To *Home nursing care*
advertisement

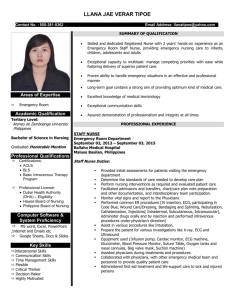
Change Management from “Home visit” To “Home nursing care” Presented by Mrs.Phensiri Atthawong, Mrs.Wasana Chungtragoon and Mrs.Nitthanan Anusornprasert From : Community Nursing Department of Songkhla Hospital, Songkhla Province, Thailand Rational the number of patients on bed are likely to increase every year (data from Continuing of Nursing care Center (COC) of Songkhla Hospital) ; 45, 80, 83 and 103 cases per 100,000 population respectively) community nurse is therefore necessary in helping on bed patients as well as their caregivers to handle their own selfcare which consequently can reduce complications and increase good life quality. According to continuous nursing model development in term of home visits, focusing on quality system as per criteria set by Bureau of Nursing council in Thailand. Objective To developed the model of home visit Caring patient at home in order to prevent any other illness conditions including complications to follow up and assess health care result as well as solve problem to achieve a better life quality in all patients, caregivers and families. Strategic of Development Model Model Development Patients’ hospital ward caring is adapted to use for patient caring at home by using Primary Care Unit (PCU) as a nurse station a patient’s home as a ward a community nurse as case manager a caregiver as a nurse’s aid community volunteer and other concerned parties as a multidisciplinary team. Visiting Team -PCU’s team member -Multidisciplinary Team ( Physician, Physio therapist, Dietician, pharmacist, etc.) -Concerned Party Network (community volunteers, Local authorities ) System Management -Set visiting system focusing on bed patients -Implement home visit flow charts -Study patients’ history of illnesses -Co-ordination with concerned party network and multidisciplinary team System model Home Visit Service -In charge system usage -pre-conference prior to home visit -Home visit > 80% (results 100%) 2.Satisfation of customers (results 97.14%) > 80% 3.Satisfaction of providers > 80% (results 94.79%) Nurse note on nursing care history of visited patients in the provided form 4.The incidence of complication in patients < 5% (result 2.8%) Nursing Care Co-ordination at home -Provision of COC in order to link caring system from hospital to community and from community to hospital Supportive Factors -Relatives and caregivers -Support multidisciplinary team through e-mail, line, skype, telephone) -Concerned party network home -Post-conference for knowledge sharing and future planning for continuous nursing care Resources -Medical tools -Community volunteers 1.The coverage of visiting patients type 3 at 5.Patients can control progression of disease and handle their own > 80% (results 94.79%) 6.Crisis Patients who need to refer has been refer in time 100% (results 100%) Conceptual Framework of Home-Nursing Care System Developme nt Teamwor k Service mind Empowerm ent “SEAMLESS Team” Achievem ent Managem Safety ent Engagem ent Life style Change Management