CCFA research priorities and Exchange
advertisement

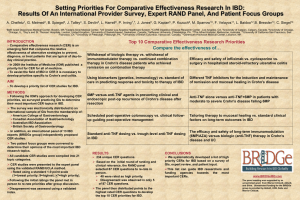
CCFA RESEARCH PROGRAMS, PRIORITIES and IBD Exchange Balfour Sartor, MD Chief Medical Advisor Marjorie Merrick Vice President, Research and Scientific Programs CCFA’s Mission and Vision Statements Mission: To cure Crohn's disease and ulcerative colitis, and to improve the quality of life of children and adults affected by these diseases. Vision: A future free from Crohn’s disease and ulcerative colitis. CCFA Has Invested $200 Million In Research Since 1967. How Have Things Changed? 1967: • Very little research was conducted in the field of IBD. • Few therapies were available (primarily prednisone and sulfasalazine, segmental resection CD, ileostomy after total proctocolectomy UC). • No genes had been identified • For many IBD patients, a stay in the hospital might run into weeks or even months. How Have Things Changed? • CCFA, NIH, medical centers and pharmaceutical companies around the world are actively conducting basic, clinical and translational research in IBD. • CCFA has supported over 1400 research grants and currently funds approximately 200 ongoing and new grants annually. • There are multiple drugs now available, including the biologics, and many experimental therapies in the pipeline. • Over 163 genes have been associated with IBD. • The average hospital stay for people with Crohn’s or colitis has been reduced to approximately 9 days. Unmet Clinical Needs in IBD (Sartor perspective, not CCFA) • Accurate prediction of disease course and response to treatment in an individual patient • Induction and maintenance of remission in patients unresponsive to or intolerant of antiTNF mAb • Induction of remission of mild to moderate ileal Crohn’s disease without steroids or biologic therapies Unmet Clinical Needs in IBD (II) • Sustained clinical remission in majority of patients that require steroids or anti-TNFs for induction • Optimal prevention of relapse in postoperative CD and pouchitis in UC • Identify clinically relevant subsets of patients with predictable clinical responses- individualized therapy. Mechanistic approach • Cure of CD and UC and prevention of onset of IBD in susceptible individuals CCFA Research • Approximately 200 active grants per year (ongoing and new awards). • Average of $16 million per year over past 4 yrs • $21 million in 2014 CCFA Research Programs Investigator- Initiated Research Grants - Senior Awards - Career Development Awards - Research Fellowships Research Resources - PROKIIDS network - Clinical Research Alliance - CCFA DNA Bank - CCFA Microbiome Bioinformatics - CCFA Data Management Center Research Initiatives - Microbiome Initiative - Genetics Initiative - RISK Stratification study - OSCCAR - CCFA Partners IBD Exchange Research Pilots - Biomarkers - Perioperative infections - Mucosal healing UC - PROKIIDS - QI CCFA Research Strategies 1. Fund the best peer-reviewed research available. 2. Train the next generation of IBD investigators 3. Help perpetuate the rapid progress in basic and clinical IBD research of the last decade by providing seed money to enable investigators to generate data to become competitive at NIH 4. Facilitate early introduction of novel technology that has the potential to lead to paradigm shifting breakthroughs into IBD research CCFA Research Strategies (II) 5. Identify host and microbial pathways that provide novel therapeutic approaches, then partner with pharmaceutical companies to develop new drugs 6. Frequently update and prioritize research goals (Challenges in IBD), then widely publicize these research priorities Challenges 2013 CCFA’s Strategic Plan for Research Chairs: Ted Denson, Dermot McGovern Genetics: Microbiome: Adaptive Immunity: Innate Immunity: Epithelial Cell Biology: IBD Diagnosis: Optimizing Therapy: Epidemiology/ Environmental Factors: Dermot McGovern, Subra Kugathasan Balfour Sartor, Gary Wu, Vince Young Theresa Pizarro, Ed deZoeten Thad Stappenbeck, Scott Plevy, Clara Abraham Asma Nusrat, Declan McCole, Christian Jobin, Charles Parkos Ted Denson, Corey Siegel, Peter Higgins Hans Herfarth, Jeffrey Hyams Ed Loftus, Mike Kappelman, Millie Long Challenges 2013 1. Define clinically relevant subsets of patients with IBD using genetic, immunologic, microbial, tissue expression, and clinical profiles (to include drug levels) that will predict aggressiveness of disease, complications and response to treatment. 2. Understand how environmental factors enhance risk of IBD through effects on microbial, epigenetic, immunologic, mucosal barrier influences – with an early focus on diet. Challenges 2013 (continued) 3. Further understand reciprocal interactions (crosstalk) between genes, microbiota, epithelial cells, innate and adaptive immune responses that determine pathways mediating mucosal homeostasis versus inflammation. 4. Determine which environmental triggers initiate, perpetuate, and/or reactivate disease. 5. Determine optimal treatment strategies through comparative effectiveness studies. Resources Identified as Essential 1. Centralized and distributable infrastructure for biobanking, data warehouse, and tissue/cell/microbial repositories for integrated human investigation. 2. Prospective cohort studies of pediatric and adult IBD patients with serial biospecimens collected throughout the course of their diseases. 3. Infrastructure to recruit and follow patients from childhood to adult life. 4. Access to data and biospecimens collected prior to and following treatment with established and novel therapeutics. Resources Identified as Essential 5. Improved tools for measuring disease activity in IBD. 6. More specific in vivo tools including humanized mice and lineage specific models for mechanistic research. 7. Availability of new methodology for improved cell lines and freshly isolated and viable mucosal cells. 8. Implementation of a series of workshops to improve IBD research methodology and promote integrative multidisciplinary approaches and resources. Research Initiatives Designed to fill important unmet needs in IBD research based on priorities described in Challenges in IBD Research: • • • • • • PROKIIDS IBD Research Network- RISK, PROTECT CCFA Partners Clinical Research Alliance Genetics Initiative Microbiome Initiative IBD Exchange Pediatric Risk Stratification Project • 26 centers have enrolled ~1100 newly diagnosed pediatric patients with Crohn’s disease (1754 overall pts: 70% Crohn’s disease, 15% UC, 5% indeterminant colitis, 10% controls • Goal: identify serum biomarkers, fecal bacteria, genes, immunologic and clinical patterns that predict at the time of diagnosis which child will develop severe, complicated vs. mild Crohn’s disease and which individual will respond to each medication • Resources: Ileal and rectal biopsies on majority of pts (Illumina deep sequencing 16srRNA), fecal samples, tissue mRNA profiling (RNA seq), all pts genotyped (Immunochip), serology, prospective serial clinical phenotyping and therapeutic responses Microbiome Consortium (2010- 2013) • 7 multi-center, multi-disciplinary consortia studying large cohorts of Crohn’s disease, UC, normal and non-IBD subjects • Explore mechanisms by which genetic influences, AIEC, Paneth cells influence intestinal bacterial composition and function, IEC/ microbial interactions, viral triggers of disease onset/ flares • Perform mechanistic studies of CD gene regulation of gut bacteria in genetically engineered gnotobiotic mice Renewal (2014-16). Prospective cohorts ileal CD & UC serially sampled (bxs, stool metabolomics), functional verification of candidate pathways to identify targets, high throughput screens for candidate drugs Microbiome: Anticipated Outcomes • Identify key microbial components that initiate and perpetuate disease • Find biomarkers that can predict disease course • Select subsets of patients that are likely (or unlikely) to respond to a particular treatment • Develop novel ways to manipulate the microbiota to both treat and prevent disease (Better antibiotics, probiotics, diets, fecal or microbial transplants) • Develop intervention strategies to prevent disease in high risk individuals (perhaps identified by their genetic and/ or microbial profiles) IBD Exchange Mission & Philosophy • Mission - create an interconnected collection of patient information, biospecimens and knowledge to advance our understanding of the causes and lead to the discovery of a cure for IBD. • Philosophy - the community who takes advantage of the resources will also contribute to building the resources by depositing their data, discoveries and newly created resources back into IBD EXCHANGE so that others can benefit from the new knowledge that has been developed. IBD Exchange Goals 1. Provide investigators with access to the resources needed to support their research. 2. Facilitate sharing of knowledge more rapidly than relying on publication in peer-reviewed journals. 3. Promote collaboration among investigators and sharing of clinical data and biospecimens. 4. Serve as an educational venue for investigators and patients with IBD. IBD Exchange Strategies 1. Collect detailed clinical information on patients with IBD including treatment, exposures, complications, outcomes from prospectively followed cohorts of adults and children with IBD, 2. Collect patient reported outcomes from prospectively followed cohorts of patients with IBD 3. Create a biosample repository containing blood, feces, urine, and tissue samples, 4. Create a knowledge environment to include a data warehouse, specialty research cores, analytic tools, educational tools for scientists, and educational tools for patients 5. Promote novel research through a peer reviewed research grants program. Prospective Cohorts Biobanks Data Repository Analytic Tools Specialty Research Cores Research Grants Year 4-5Exchange Study “y” “PROTECT” SHARE / VEO / Other HT Projects “RISK” “Microbiome” Partners 2 Other CCFA studies Exchange cohort “Genetics Initiative” OSCCAR Substudy “x” Spectrum of Initial IBDEX Cohorts Patient Reported Outcomes Clinical Activity Indices Biosamples Newly diagnosed pediatric CD Partners 2 RISK & VEO RISK & VEO Newly diagnosed pediatric UC Partners 2 Protect & VEO Protect & VEO Established adult IBD Partners 2/ PCORI Exchange Cohort & SHARE Exchange Cohort, SHARE, Microbiome Newly diagnosed adult IBD OSCCAR, Partners 2 Exchange Cohort, PCORI OSCCAR & SHARE Exchange Cohort, OSCCAR & SHARE Community based International Referral center based Data Warehouse and Learning Environment Ancillary study investigators use data and samples IBDEX cohorts generate data and samples Investigators funded by CCFA and Helmsley generate data and samples IBD EX Knowledge Center All newly generated data remains linked to the samples that were used to generate the data Ancillary study investigators generate new data