Public Health - National Information Governance Board for Health
advertisement

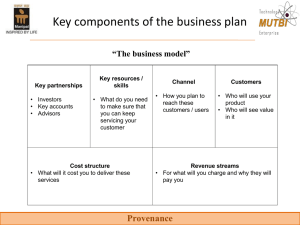
NATIONAL INFORMATION GOVERNANCE BOARD FOR HEALTH AND SOCIAL CARE NIGB NIGB IG Collaborative Workshops The Reality of Delivering the Information Revolution Break out Sessions Consultation #NIGB #HSCIG Leeds – Birmingham - London Public Health in Transition NIGB Information Governance Collaborative Workshops 2012 Jürgen Schmidt (jurgen.schmidt@dh.gsi.gov.uk) Robert Kyffin (robert.kyffin@dh.gsi.gov.uk) Public Health England Transition Team Presentation overview • • • • • • • • Roles, responsibilities and relationships in the new health and social care system Information requirements of public health Information governance framework: current arrangements, issues and actions Local public health intelligence Commissioning landscape and the roles of PHE and the NHSCB Public health intelligence business model Issues for PHE Issues for Local Government and the NHS Public Health England – role and functions • • • • Responsible for delivering a new integrated public health service providing support and expert advice to national government, Local Authorities and the NHS PHE will work with partners across the health and social care system to: – deliver, support and enable improvements to health and wellbeing, particularly in the areas set out in the Public Health Outcomes Framework – lead on the design, delivery and maintenance of systems to protect the population against existing and future threats to health PHE’s overall mission is to protect and improve health and wellbeing, and reduce inequalities in health outcomes Three main business functions: delivering services, leading for public health, and developing the public health workforce Public Health England – structure and relationships • • PHE will have a national headquarters supported by a network of regions (aligned to the NHSCB and CLG regions), centres (broadly comparable to the NHSCB area teams) and a nationally managed but regionally distributed network of evidence and intelligence teams – final configurations and functions all to be decided Relationship with the NHSCB: – a Compact is being negotiated to establish collaborative strategic goals and working relationships – PHE will provide advice on NHS priorities and service specifications for public health services such as screening and immunisation – PHE will provide a public health and information and intelligence service to the NHSCB Public Health England – structure and relationships Relationship with Local Government: • DsPH and their teams in Local Authorities are taking on a wide range of public health responsibilities including: – – – – • producing the Joint Strategic Needs Assessment providing a healthcare public health advice service ensuring health protection plans are in place commissioning NHS Health Checks and some clinical services such as sexual health and child health services – scrutinising and challenging NHS performance eg. screening PHE will provide advice and support in undertaking these responsibilities through national leadership role and provision of the local ‘proposition’ ie. support offer Public health uses of identifiable information • • Public health uses identifiable information in three main ways: – Surveillance: to monitor current and emerging threats to health, identify trends in health behaviours and risk factors, detect unusual patterns of disease, monitor outcomes – Health intelligence: to provide public health practitioners, commissioners, policy makers and the public with information and intelligence on the challenges, threats and risks to health – Direct provision and quality assurance of services: to manage the delivery of high quality and safe screening, cancer, immunisation and other public health services Identifiable information is required to avoid double counting, enable the use of capture-recapture techniques, link records, and support service delivery Public Health England – information governance framework • PHE sender organisations have the following legal and statutory permissions to use identifiable information: – Cancer screening: the NHS bowel, breast and cervical cancer screening programmes have s251 approval – Cancer Registries: cancer registration is covered by Section 2 of the Control of Information Regulations 2002 – National Treatment Agency: NDTMS data is collected with consent – Non-cancer screening: the NHS Abdominal Aortic Aneurysm and NHS Sickle Cell and Thalassaemia Screening Programmes have s251 approval; other programmes such as the NHS Newborn Hearing Screening Programme collect data with consent – Other disease registers: the English Congenital Anomaly Registers have s251 approval Public Health England – information governance framework (cont.) – Health Protection Agency: the Public Health (Control of Disease) Act 1984 (as amended by the Health and Social Care Act 2008) and its associated Regulations (2010), the Sexually Transmitted Diseases Directions 2000, Section 3 of the Health Service (Control of Patient Information) Regulations 2002, the Health Protection Act 2004, the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010, and the Health Protection (Notification) Regulations 2010 cover health protection uses; specific HPA programmes also have s251 class approval Public Health England – information governance challenges • Key information governance challenges facing public health: – Omissions from the framework: eg. cancer and non-cancer screening programmes do not have statutory support to use identifiable information for service delivery so rely on s251 – Discontinuities within the framework: eg. ambiguities in the legal interpretation of the Sexual Health Directions 2000 have led NIGB to state that s251 support cannot apply to the use of data on sexually transmitted diseases by the HPA – Issues of interpretation and application: eg. “other risks to public health” in the Control of Patient Information Regulations 2002 narrowly interpreted to mean health protection rather than a wider range of public health risks – Unintended adverse impacts of the framework: eg. evidence from the NHS Dental Epidemiology Programme that move to an explicit consent model has reduced response rates Public Health England – information governance requirements • • • Secure legal basis needs to be established for defined public health uses of identifiable information Balance to be struck between public benefits and public disbenefits of public health access to identifiable information Work currently underway in PHE to develop the information governance framework: – PHE working with DH, NHSCB and other partners to propose amendments to Regulations 2 and 3 of the Health Service (Control of Patient Information) Regulations 2002 – PHE working with DH, NHSCB and the HRA on the legacy of s251 and the future advisory and decision functions – PHE working with HSCIC on the Code of Practice for Handling Confidential Information (covering anonymisation, disclosure, retention etc. standards), and on safe haven arrangements and data linkage services Context for local public health intelligence work • • What are the relevant changes? – Physical move and changed functions of DsPH and their teams – Local Authority public health responsibilities – Local ‘proposition’ ie. support offer Formal requirements: – NHS planning guidance for 2012/13: To agree arrangements on public health information requirements and information governance by September 2012 – PHE transition guidance checklist item: Are plans in place to ensure access to IT systems, sharing of data and access to health intelligence in line with information governance and business requirements during transition and beyond? Business continuity – what does the future look like? • • Emerging commissioning landscape – Functions and data flows, including data sharing and the integration of health and social care data – Changes to the IT environment, including the NHSCB DMICs – Changes to the information governance environment PHE contribution to the system – Functions: data requirements, informatics (governance, standards and quality), surveillance strategy – Products and tools around data, evidence and experience (PHOF, DPH Annual Reports, JSNAs) – Partnership work with IC, NICE, ONS – Guidance on use of both PHE and non-PHE products – Responsive ad hoc service based on PHE products and other relevant sources of public health intelligence System connectivity Home office DCLG others DWP HMRC GSI Government gateway PSI gateway GCSX Gateway Citizen Local authorities N3 CJSM PNN others The Commissioning Intelligence Model NHSCB Commissioning Intelligence Model Types of Services Tools/Data Types of Services S8.01: Demographic forecasting & disease trends (Provenance: D8.01: Programme budgeting (comparative spend on disease conditions) & marginal analysis, PBMA Atlas, SPOT, SHAPE (Provenance: HB) D8.02: Health investment packs, QIPP (Provenance: HB) S1.01: Health needs / Joint Strategic Needs Assessment/ Impact assessments (data & analytical input) (Provenance: AF/WS290911) HB) S8.04: Forecasting and future projections of expected activity. (Provenance: HB) S8.05: Cost Benefits analysis of current activity vs. alternatives (Provenance: HB) S8.06: Strategic secondary analysis of 'How Healthy' and 'How much?' (Provenance: HB) D8.03: Pathway modelling inc ROI calculators, return on investment tools (Provenance: HB) D8.04: Results and secondary analysis of other questions, design making support etc (Provenance: HB) D8.05: Quality of life & well being measures e.g. QALYs (Provenance: CH181011) D8.06: DH Programme Budgeting tool / Spend and Outcome Tool (Provenance: CH181011) S8.07: Track and react to patient expectation (Provenance: HB) S8.08: Manage Programme Portfolio (Provenance: CH181011) S8.09: Programme budgeting (comparative spend on disease conditions) (Provenance: CH181011) D8.07: Patient expectation information (Provenance: CH181011) Q8.01: Are our strategic objectives aligned across the health economy inc social care? Q8.02: What will be the impact of demographic and disease pattern change? Q8.03: How can we make QIPP savings of £XXXm? Provenance: HB Provenance: WS270911 Provenance: HB (Provenance: AF) S1.05: Geographic analysis and mapping, socio-demographic analysis. (Provenance: AF/HB) S1.06: Identification of at-risk groups (e.g. Communities (inc Travellers), Carers etc) (Provenance: Auth) S1.07: Informing the public about keeping healthy, prevention resources (Provenance: HB/CH) S1.08: Research, surveys, audits, peer reviews (Provenance: HB/ WS290911) S1.09: Managing needs of Stakeholders (e.g. Care Home, Community, Health Education) (Provenance: WS290911) D1.06: Deprivation indices (Index of Multiple Deprivation). (Provenance: AF) D1.07: Access to and familiarity with wide range of Public Health data sources, Benchmarking and comparison tools (e.g. NHS Atlas of Variation, NCHOD, Local tools). (Provenance: CH181011) D1.08: Dynamic ethnicity data analysis across all aspects of care. Wider equality indicators including disability, sexual orientation etc (Provenance: HB) D1.09: Data on wider determinants, social service, HPA (Provenance: HB) D1.10: Predictive disease monitoring (Provenance: WS270911) Q1.01: How healthy/ unhealthy is my population relative to benchmarks? Q1.02: What health conditions are changing most? Q1.03: Who is at greatest risk of disease/acute admission to hospital? Provenance: AF/WS290911 Provenance: V10 Provenance: AF/WS290911 Provenance: HB Types of Services S7.04: Performance reporting. (Provenance: AF) S7.05: Providing comparative outcome monitoring inc Patient and Public Data (Provenance: HB) S7.06: Production of Board level reports, presentations and profiles (Provenance: CH181011) D7.01: Performance & Public Health metrics, frameworks and dashboards (Provenance: AF) D7.02: Activity & cost baseline and tracking data (Provenance: AF) D7.03: Impact analysis & evaluation using statistical tools (Provenance: AF) D7.05: Public Health Observatory tools including survey tools (Provenance: HB) D7.06: Data outputs from all other dimensions (as appropriate) (Provenance: CH181011) D7.07: Data required for Programme Gov inc Benefits Mgmt, Plans etc (Provenance: CH181011) Q8.09: What barriers exist that prevent change (e.g. org/cultural)? Provenance: WS270911 Q7.01: When a service change is implemented, what was the outcome, cost and quality for this and to other services? S6.03: System-wide activity & cost modelling (Provenance: AF) S6.06: Review evidence base (e.g. National Comparators, NICE, etc) (Provenance: V13) S6.07: Capture & manage stakeholder feedback/outcomes Provenance: AF Provenance: WS270911 Provenance: AF Q1.07: Who would benefit most from a disease management programme? Q1.08: What causes patients most distress? Provenance: WS270911 8. What are our future plans? Reduce unmet need by anticipating future priorities and improving decisions about resource allocation, by ensuring planned services reflect changing needs and demands of local population Q7.08: Did we meet our targets and can we sustain them? Provenance: AF Q7.03: What's the combined impact of all our interventions for patients, the services & health economy? Q7.09: What are the benefits of the changes? Q7.06: Have we reduced inequalities? embedded in the cycle of continuous improvement to improve patient experience Q6.01: What would be the impact, in activity flows and costs, of making a proposed change to a clinical pathway? 6. How could things be better? Q6.07: What are our drivers for change and have we engaged with stakeholders (inc Patients) Provenance: AF Q6.02: What will be the combined impact, in cost and activity, of a whole set of service changes and productivity measures? Developing new pathways and/ or decommissioning services to improve safety, quality, effectiveness of care and maximise financial benefit Provenance: WS270911 D6.07: Data outputs from all other dimensions (as appropriate) (Provenance: What questions do we need to answer? 5. Are my providers delivering what they agreed? Improve commissioning Provenance: HB Provenance: AF decisions through better information and information analysis Q6.05: Do we need to procure services from alternative providers, or work in partnership with other stakeholders to be more efficient for provision and procurement? 2. What's really happening in this system? Information available at right time and to the right person to protect the vulnerable and ensure the right care is given to reduce duplication and improve integration of care D6.09: Staff surveys, appraisals, complaints, incidents and SUIs (Provenance: Provenance: AF/WS290911 Provenance: CCG 3. How Much? Improved financial information (including budgeting and planning) to ensure resource is given to appropriate care provider for the treatment given and ultimately there is better transparency of financial flows to support improved commissioning decisions Provenance: AF Q3.08: What is the projected liability for our referred population? Provenance: WS021211 4. How do we Compare? S5.05: Contract development (Provenance: MT) S5.06: Performance Management and support for service improvement (inc Negative impacts and Data Management) (Provenance: MT) S5.07: Utilisation reviews, PbR Audits, Clinical Decision Support (Provenance: WS290911) S5.08: Basic budget reporting (Provenance: CH181011) S5.09: Contract validation, challenge (Provenance: CH181011) S5.10: SUS validation with GP Practice Systems (Provenance: CH181011) Q3.02: How much do individual service- lines/ pathways cost compared to budget? Q3.03: Is cost aligned to volume, quality and outcome? Types of Services S3.01: Service-level costing (e.g. by Specialty, HRG chapter, Diagnostic chapter) (Provenance: AF) S3.02: Budget planning, development & forecasting (Provenance: AF/WS290911) S3.03: Budget Reporting & Variance analysis (Provenance: AF) S3.04: Price verification (provider costings) & reconciliation to contract, automated invoice validation (Provenance: AF/CCG) S3.05: Comparative Provider cost analysis (Provenance: AF) Provenance: V13 Challenge our current state through proactive benchmarking and comparison in order to improve clinical outcomes Q3.09: How much are we spending on inequalities? Provenance: WS290911 Q3.04: Are we maximising value for money? (e.g. community provision vs. acute care) Tools/Data D3.02: Current and historic Provider Activity and Cost data-sets (SUS & Local Contract Mgmt systems) (Provenance: V10) Q4.01: Where is there clinical / activity / cost / outcome variation vs local, national, international, best practice? Q5.06: Can we distinguish between Provider 'pull' and Primary Care 'Push' Q5.07: Are Providers sending datasets to agreed standards and frequency? (If not, are there sanctions in place?) Tools/Data D5.01: Data warehouse integration and reconciliation of Activity/Cost and Provider contracting reports (Provenance: AF) D5.02: Contract Monitoring reporting by Provider (Provenance: CH181011) D5.05: LA, Primary care and Voluntary/third sector (Provenance: WS270911) D5.06: Referral Data (Provenance: CH181011) D5.07: CQUINS (Provenance: CH181011) D5.08: Insight into provider sustainability (Provenance: V10) D5.09: Patient Feedback (Provenance: V12) Q4.02: Are we delivering national standards of care for: patient experience, quality and outcomes? D3.03: Tariff / Pricing tables, PBR rules and algorithms (local and national), Prescribing costs (Provenance: CH181011) D3.05: Robust timely referral activity Provenance: AF/WS290911 (Provenance: WS290911) D3.07: Reference Cost Data (Provenance: CH181011) Q4.05: How do we compare for value for money, outcomes and productivity against similar areas/ best practice over time? Q4.04: Do current pathways reflect evidence-based good practice? Provenance: AF Provenance: AF/WS290911 Provenance: V13 Types of Services Tools/Data S4.01: Practice level, regional, and national benchmarking of disease prevalence, activity, productivity and costs. (Provenance: AF) D4.01: Age-sex-deprivation standardised comparative data at Practice level for commissioned activity (inc practice specialism). (Provenance: AF) D4.02: Primary Care data extracts providing integrated analysis with Acute activity, e.g. prevalence rates vs. Admissions. (Provenance: AF) Provenance: CCG S5.04: Provider level-analysis of ‘how much’ and ‘how good’? (Provenance: AF) Provenance: AF/WS290911 Q3.07: Where are the most severe cost pressures? D3.06: Referral templates with expected costs (Provenance: CH181011) Q5.04: What service lines are above or below plan why? Types of Services S5.03: Invoice validation, challenge (Provenance: CH181011) Q3.01: How much is my budget? How much am I spending compared to plan? Provenance: WS270911 Provenance: V13 S5.01: Analytical support to Contract monitoring & analysis (Provenance: AF) S5.02: Provider activity validation & Data Quality review (Provenance: AF) Provenance: AF V10) Q5.02: What elements of the billed activity can we challenge? Q5.05: Are providers overlooking agreements on Threshold Management? Provenance: V12 Q3.06: Is activity being priced at the correct amount? (Provenance: WS021211) Provenance: AF D3.01: SUS reporting & analysis webservice, including Budget reports. (Provenance: Provenance: V13 Q5.08: Do our provider contracts reflect patient requirements? Provenance: AF Q2.06: How much random variation in activity do we observe? Provenance: AF V10) D6.10: External information e.g. Market intelligence (Provenance: V13) Q2.05: Where are the bottlenecks? Provenance: V13 Q5.03: Are providers delivering on serviceimprovement, quality (cquins) patient experience and waiting-times targets? (Provenance: V10) Q2.10: To what degree are patients able to make informed decisions about their care? Q5.01: What is the current performance against plan? Provenance: MT/HB/WSS290911 D6.08: Stakeholder feedback including external sources such as Social Media and Public Enquiries D2.03: Current, historic and planned Provider Activity and Cost data-sets (SUS & Local Contract Mgmt Systems e.g. Maternity, Mental Health, Local Auth etc) (Provenance: V10) D2.05: Waiting times/list data (Provenance: AF) D2.06: Patient level datasets with updates inc: decisions made in secondary care – reasons for treatment/changes/referrals/delays /test results and outcomes (Provenance: HB) D2.07: External Sources such as Social Media Provenance: AF Q6.06: How do we compare with evidence and guidance for process, outcomes and patient experience? Q6.03: Would 'Scenario A' improve patient flows and productivity more than 'Scenario B'? CH181011) D2.02: SUS data, including acute activity & costs, referrals with clinical reason, CAB, 'PatientJourney' analysis. (Provenance: CH181011) Provenance: AF/WS290911 Provenance: AF (Provenance: AF/HB) (Provenance: WS270911) Q2.04: What are the current flows and pathways and are patients using the right ones? Provenance: CCG 7. What difference have we made? Ensuring patient feedback is Provenance: WS290911 Provenance: HB Tools/Data D2.01: Near/real time information - activity & financial for A&E, OOHs, MIU, Acute and Community Admissions etc (Provenance: CH181011) Provenance: AF Q2.09: What is the impact of patient choice on Provider volumes? Provenance: V12 Provenance: HB S2.13: Track patient experience (Provenance: CH181011) Q2.03: Is demand really going up? By how much? Q2.07: What is the demand today for urgent care, and who do I need to target to keep out of hospital? Provenance: AF S6.08: Clinical governance and complaints handling (Provenance: V10) Tools/Data (Provenance: WS290911) S2.12: Management of Urgent Care Monitoring/ Dashboards (Provenance: CH181011) Q2.02: How long are patients waiting for treatment? 1. How Healthy? Reducing health inequalities and improving health outcomes now and in the future Q7.10: What is the impact of change on other services & stakeholders? Q7.05: Have we improved outcomes? S2.09: Indicators to track progress throughout pathways reasons/decisions for referrals, patient experience and outcomes. Provenance: AF Provenance: HB Provenance: AF/WS290911 (Provenance: HB) Provenance: AF Provenance: WS270911 Provenance: AF D6.03: Forecast analysis and planning projections (Provenance: AF/HB) D6.04: Service structure audit and improvement support. (Provenance: AF/HB) D6.05: Prescribing decision support data (Provenance: HB) D6.06: Capture & processing of patient experience and outcomes throughout pathways, inc PROMS AF) S2.07: Provide access to patient medical records Q2.01: Why have we got financial pressures? Q1.10: What are the preventable conditions contributing to our premature mortality? Provenance: WS270911 Provenance: AF/HB/WS290911 (Provenance: WS290911) D6.01: Pathway data (Provenance: AF) D6.02: Contract activity and cost Types of Services S2.01: Trend and statistical analysis (activity, cost, SPC) (Provenance: AF) S2.02: Capacity and demand analysis, patient flow modelling, waiting times analysis (Provenance: AF) S2.05: Analytics support to Clinical audit. (Provenance: Provenance: AF Q1.09: What proportion of disease is avoidable? Provenance: HB Types of Services Q1.06: Who are the sickest people and where do they live? Provenance: CH181011 Q7.07: How did our patients rate their experience of our services? S6.01: Pathway & scenario modelling (inc Audit of Admission thresholds and service structure) (Provenance: AF) S6.02: Contract modelling (Provenance: AF) Q1.05: What diseases kill most people and which are the biggest burden? Provenance: WS290911 Q8.10: Are our investments distributed across all sectors to best meet the needs of our population? Q7.02: Can I isolate the 'cause and effect' of an individual initiative? Tools/Data Q1.04: How is the local population going to change in future? Provenance: HB Q8.07: Have we got the balance correct between national, local and patient expectations? S7.01: Programme and project monitoring. (Provenance: AF) S7.02: Providing comparative cost and activity monitoring (Provenance: AF) S7.03: Metrics reporting. (Provenance: AF) Q8.06: What activity should we contract for to deliver the service changes / cost efficiencies needed? Q8.05: Given our budget, how can we decide how much to invest/disinvest in services? Provenance: HB The CIM Model is a consolidated view of the different types of commissioning intelligence requirements needed to support evidence based commissioning decisions S1.03: Demographic forecasting & disease trends. (Provenance: AF) Q8.04: How will changes in technologies (IT, drugs etc) impact us? • Tools/Data D1.01: Population, migration, birth, mortality and morbidity statistics and projections (ONS, Exeter, QOF, Primary Care, SUS, Prevalence modelling tools, Census) (Provenance: AF/WS290911) D1.02: Public Health Data Observatory / Local Information Systems / JSNA / Cancer Registry / Qualitative Data inc Voluntary & Third sector (Provenance: AF/HBWS290911) D1.03: Risk Stratification tools and models: Patients at Risk of Readmission (PARR), Combined Predictive Model, Adjusted Clinical Groups. (Provenance: AF) D1.04: Socio-demographic classification system (e.g. Mosaic, Health foundations DH segmentation tool). (Provenance: AF/WS290911) D1.05: Mapping and geo-spatial software S1.02: Risk profiling & prediction. (Provenance: AF) Overarching Concepts O0.01 Interpretation, contextualisation, exploitation and stakeholder communication O0.02 Data collected at patient level O0.03 Holistic Analyses - Full System view rather than isolated segments O0.04 Flexible tariffs O0.05 Master Data Administration (inc Common currencies & agreed standardisation techniques) O0.06 Timeliness and quality of data O0.07 Data definitions and standards O0.08 Interoperability O0.09 Knowledge Management O0.10 Integrated ways of working O0.11 Development of Metrics O0.12 Simplify presentation appropriate to audience Draft for Discussion Only S4.02: Analysis and presentation of productivity indicators by programme / project. (Provenance: AF) S4.03: Clinical Pathway mapping and modelling and cost comparators (Provenance: AF/ WS290911) S4.04: Providing evidence and information on comparative health outcomes. (Provenance: AF/WS290911) S4.05: Statistical analysis of variation and correlations e.g. Statistical Process Control (Provenance: CH181011) D4.03: Comparative benchmarking tools (e.g. QOF Data sets, NHS Comparators, NHS Atlas of Variation, Better Care Better Value indicators). (Provenance: CH181011) D4.05: Benchmarked GP referrals analysis. (Provenance: AF/HB) D4.06: Practice profiles (Needing national standards) (Provenance: HB) D4.07: National Guidance, PROMS, Utilisation reviews (Provenance: CH181011) Filename: Commissioning Intelligence Model V13.vsd Version Date Comment 1. Aug 11 Original from Andrew Fenton 2. 15/9/11 Added comments from Ming Tang, Helen Brown and responses to the IFC document 3. 21/9/11 Added comments from Shahid Ali and benefits from Jo Butterfield 4. 27/9/11 Tidied version for workshops 5 28/9/11 With comments from London Workshop 6. 14/10/11 Added comments from workshop and consultation feedback 7. 19/10/11 After linking data to services (CH & HB) 8. 28/11/11 Q8.3 to include QIPP 9. 5/12/11 Amendments after CSO workshop on 2/12/11 10. 9/12/11 Amendments after ref group review Version 11. 12. 13. Date Comment 14/12/11 Amendments to support Business Analysis Team 14/12/11 Further amendments after CSO workshop on 2/12/11 19/1/12 Text changes from Gavin McIntosh Business model Data management capabilities could be provided by specialist integration centres supporting CSSs and CCGs using an integrated commissioning data model Secure Data Extraction & Transfer External Data Sources SUS GP MH Community Conformed Master Data Mgt Data Upload & Integration Integrated Data Store ETL Layer Data Validation & Processing Other... 1. Multiple Data Sources; Extract, Load& Transfer: • National (secondary usage) • Direct • Agreed Standards & business rules for cleansing & validation Business Intelligence Layer Data & Reports Applica tions Analysis 2. Data Integration & Normalisation • Conformed dimensions used to link data sets • Stored data can now be ‘mined’ for BI reporting, benchmarks & available for other applications • Requires dimension schemas (logic for how data can be linked) • Data linkages relate to key questions for BI Security & Presentation Layer • Access Layer - B2B Users - End users 3. BI Presentation & Security Layer • User friendly, timely and flexible data elements & reports • Configurable analysis and comparative benchmarks • Applications that support decision making & workflow • Security layer reflects user access rights / role authorisation National Bodies Sub-national National incl: NHSCB, PHE, Research, Commercial, CQC, Monitor & Public National Data Feeds IC Safe haven Local & National Data Feeds DMIC x ~10 Safe haven Small no CCGs doing own intelligence Local DMICs may also provide data to wider stakeholders CCGs CCG x~250 CSS X~25 LAPH CCG X~150 Issues for Public Health England • • • • • • • PHE contribution PHE ‘proposition’ to support local areas PHE organisational design Information governance National data requirements PHE advice and input to the NHS Commissioning Board PHE evidence and intelligence teams and the Health & Social Care Information Centre NATIONAL INFORMATION GOVERNANCE BOARD FOR HEALTH AND SOCIAL CARE NIGB NIGB IG Collaborative Workshops The Reality of Delivering the Information Revolution Break out Sessions Consultation #NIGB #HSCIG Leeds – Birmingham - London Information: to share or not share? Information Governance Review Karen Thomson Information Governance Lead 21 Review overview • Scope – when consent needed, how record consent / dissent, ensuring a secure basis in law for processing, IG in the new landscape • 15 panel members different backgrounds • Evidence gathering – verbal, written, lit review – thematic • Questions for direct care and commissioning on website – www.caldicott2.dh.gov.uk 22 Headlines - Direct Care • Agreed common terminology would be helpful – CHRE volunteered to lead • Clarity about when the social worker is part of the care team and covered by implied consent • When non-registered professions e.g. HCA are covered by implied consent • A better understanding of what is within the social contract of implied consent • And of the need to make this explicit to patients and service users 23 Headlines - Commissioning • Need for large quantities of data to create an innovative culture • Commissioning Intelligence Model will involve setting up CSSs and DMICs & access to PID • Desire to make IG an enabler – information is an asset – IG adds value thro data quality and protecting this asset 24 Headlines - Commissioning • Role of CQC – not an IG regulator – context of quality of care and managing clinical risk only • Consideration of the future of the toolkit & usefulness for commissioners • Lack of clarity about data controller / data processor relationships 25 Inputting to the Review • Any questions about the Review? • • • • Dates for evidence sessions on website Public Health session – yesterday Adult Social Care – 4 July Manchester Face to face sessions to end of October – written evidence over the summer • 3 questions sent in advance and in your pack for you to consider • Capture key elements and include in a report on this event to the IGR Panel 26 Questions asked • Your key concerns around IG in future? • Concerns are you hearing from patients, service users and carers? • Concerns from H&SC orgs, clinicians, practitioners & researchers? • Your concerns about the use of identifiable data for purposes other than direct care 27 Thank you! 28 NATIONAL INFORMATION GOVERNANCE BOARD No such thing as a free lunch NIGB • First break (11-11.30) – MetaCompliance: room 3 (ground floor) – Egress Switch: room 145 (1st floor) – FairWarning Audit: room 123 (1st floor) • Lunch break (1.30 – 2.00) – Imprivata: room 3 (ground floor) – Mastek: room 123 (1st floor) NATIONAL INFORMATION GOVERNANCE BOARD FOR HEALTH AND SOCIAL CARE NIGB NIGB IG Collaborative Workshops The Reality of Delivering the Information Revolution Break out Sessions Consultation #NIGB #HSCIG Leeds – Birmingham - London