Brigid McCaw
advertisement

Incorporating Behavioral Health in
the EHR to Improve Care
Insitute of Medicine | November 25, 2013
Brigid McCaw, MD, MS, MPH, FACP
Medical Director, Family Violence Prevention Program
The Permanente Medical Group
Health Risk Factors 2.0
Behavioral Health
is essential to health
Prevention works
People recover
Treatment is effective
Substance Abuse and Mental Health
Services Administration (SAMHSA)
BIG FOUR for Primary Care
Depression
Anxiety Disorders
Substance Misuse
Family Violence
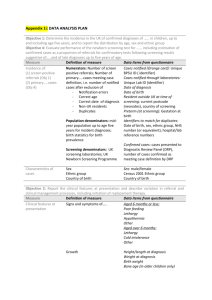
Identifying Depression and Anxiety
Symptoms of depression, anxiety, and functioning
problems combine to yield a “Global Distress Score”
Adult Outcomes Questionnaire (AOQ) includes
PHQ-9, GAD-2 and functioning items
Serves as both screener and progress monitor
Available in paper, on-line, or by secure message
Used in adult medicine, women’s health, specialty
mental health, and health education classes
Adult Outcomes Questionnaire (AOQ)
Transition in Quality Measures:
From Process to Outcome
Screening for
Depression
Diagnosis +
Treatment Contacts
Treatment +
Symptom Reduction
Treating to Target,
Monitoring over Time
Screening, Brief Intervention, and
Referral to Treatment (SBIRT)
“Alcohol as a Vital Sign”
Began June 2013.
All adult primary care patients (≥ 18 y.o.)
now screened annually with evidence-based
screener.
Physicians provide brief advice or referral to
Chemical Dependency treatment as appropriate.
Alcohol Screening: prompt in EHR
Logic: Will appear once a year (or at six months
if prior positive screening ). The first question is
gender & age specific.
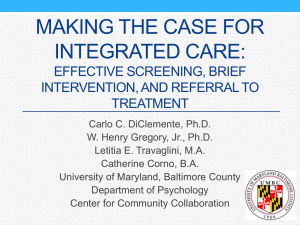
Alcohol Screening Questions
Sensitivity/ Specificity at detecting Unhealthy Use: 82% / 79%
Smith, 2009, J Gen Intern Med
NIAAA, 2005 “Helping Patients Who Drink Too Much”
Alcohol SBIRT Workflow
Medical Assistant Screens for Risky Drinking
Positive:
Physician sees screening
results; screens for dependence
with 2-question screener*
Dependence Screening is
Positive: Physician refers
patient to Chemical Dependency
treatment for further
assessment/ possible treatment
*Vinson, 2007
Negative
Dependence Screening is
Negative: Physician discusses links
between unhealthy drinking and
medical conditions, provides brief
advice to cut back to low-risk limits
BIG FOUR for Primary Care
Depression
Anxiety Disorders
Substance Misuse
Family Violence
Comparison to Other Life-Threatening
Conditions Affecting Women
In the US, each year
New cases of breast cancer[2]
211,000
Number of women dying from
cardiovascular disease[3]
484,000
Women who are injured from IPV[4]
2,000,000
IPV screening and counseling should be
core part of women’s health services
Women’s Preventive Health Care Services Committee
Universal screening for childbearing-age
women recommended
The KP Systems-Model Approach
Inquiry and
Referral
On-site
Services
Leadership
and
Oversight
Supportive
Community
Environment
Linkages
“Making the right thing easier to do”
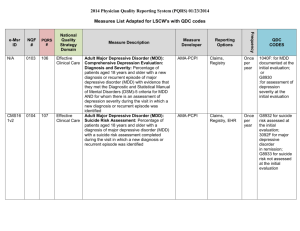
8-fold Increase in IPV Identification
Largely in primary care and mental health departments
Members Diagnosed with Intimate Partner Violence, 2000-2013
8090
{
5,000
4,500
Emergency Dept. & Urgent Care
Mental Health
4,000
Primary Care
3,500
3,000
2,500
2,000
1,500
1,000
{
500
1022
0
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Improving IPV Inquiry
Reminders embedded in Progress Note
Improving IPV Documentation,
Intervention & Referral
Smart phrases (clinic note with essential elements)
Smart set (includes note, orders, referral, followup)
Danger/lethality assessment questionnaire
Care Pathway for ED, primary care and MH
Facility specific referral protocol
Intranet resource site: “abuse and assault website”
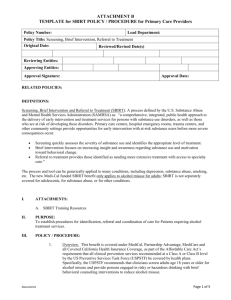
Abuse and Assault Site Connected to EHR
Online Training Tools for Clinicians
BH in Primary Care Must Address
Clinician AND Patient Concerns
The doctor:
– How do I ask about BH issues?
– What do I do when the answer is “yes”?
The patient:
– If I disclose, what will happen ?
– How will this benefit my health?
Documentation of BH Issues in EHR
Concerns: safety, privacy, stigma, visibility, discrimination
Benefits:
Facilitates coordination of care
– Prompts for follow-up and ongoing intervention
– Allows other clinicians to reinforce intervention
– Allows other clinicians to better understand what may
underlie current medical conditions and adherence
Safety
Normalizing, removes stigma
What BH issues need to be next?
Adverse Childhood
Experiences
Adult Abuse and
Trauma
What should that look like?
Integrated BH “screening” tool that
has branched logic and is interactive
Provides information for clinician
and to patient
Contact Information
Brigid McCaw, MD, MS, MPH, FACP
Medical Director, Family Violence Prevention Program
The Permanente Medical Group
Brigid.McCaw@kp.org
510-987-2035
Patient Education:
Exam Room Poster