Systematic TB screening: Operational
research - Enhanced contact
investigation of smear-positive
tuberculosis patients in Mongolia
J. Narantuya, Technical officer on HIV, AIDS, STIs,
Tuberculosis and Hepatitis, WHO Mongolia
The ninth Technical Advisory Group and National TB
Managers meeting
Manila, Philippines
9-12 December 2014
CONTENT
•
•
•
•
•
•
•
Background
Objectives
Methods
Implementation
Preliminary results
Policy implications and future directions
Acknowledgement
BACKGROUND
• Prevalence of TB in 2013 (includes HIV+TB)
254 per 100,00 population (Global TB report,
WHO 2014)
• Current practice is passive contact
investigation
• Contact investigation form is not used
OBJECTIVES
1. General objective
• To assess impact of enhanced contact investigation through introduction of
active home-visit and new recording and reporting forms in Ulaanbaatar,
Mongolia
2. Specific objectives
To describe screening coverage of household TB contacts
To determine prevalence of TB disease and latent TB infection among
household contacts
To determine secondary attack rate of pulmonary TB among household
contacts
To identify risk factors for TB disease and latent TB infection among
household contacts
To develop standard operating procedures (SOPs) for contact investigation
METHODS
• Study design
– Cluster randomized control trial
• Study area and population
– 8 districts of Ulaanbaatar city (capital) have been
selected randomly: 4 intervention and 4 control
districts
– Target population: New smear positive pulmonary TB
patients who are diagnosed and notified at district TB
dispensary and their contacts
– 460 index cases and 1536 contacts were planned
METHODS
• Eligibility criteria
– Newly diagnosed smear-positive TB patients
– A household contact is defined as any person staying in the
same household with index case for more than 3 months
before the date of diagnosis of index cases
– Informed consent
• Excluding criteria:
– index patients who are less than 15 years of age;
– index patients who have a history of TB in the family
– index cases who have no household contact (living alone).
IMPLEMENTATION
IMPLEMENTATION
• Training of health providers
• Advocacy meetings with district health authorities
• Newly developed individual contact investigation
form
• Questionnaires:
– For index case
– For household
– For contacts
• Diagnostic tools:
– Sputum smear microscopy
– Tuberculin skin test
– X-ray
PRELIMINARY RESULTS: Index
cases and contacts
Male 278 (55.7%)
80
60
0
20
• Housing
40
•
Number
Index (N=499)
• All smear-positive cases
> 15 years in 8 districts
100
Age distribution of smear−positive index cases
– House 157 (31.4%)
– Apartment 149 (29.8%)
– Ger 172 (34.4%)
15−19
20−29
30−39
40−49
50−59
60+
Age group
150
100
50
0
Number
Contacts (N=1437)
• Average 3.8 per index
• Male 632 (44.0%)
200
Age distribution of contacts screened
<05
05−14
15−24
25−34
35−44
Age group
45−54
55−64
65+
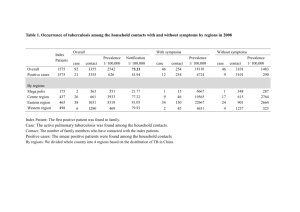
Yield
by (contact)
age
group
Yield of contact
investigation,
by contact
age group
15
●
●
All forms
Smear−positive
●
10.2 %
Yield (%)
10
●
5
●
●
●
●
0.9 %
●
0
<05
05−14
Children
15−24
●
●
2.5 %
●
●
●
25−34
Age group Adults
35−44
45+
1.0 %
Risk factors (determinants of yield)
Risk factor analysis
• Index factors
• Household factors
• Individual factors
Index factors
(preliminary)
• Index aged 30-49
• Unemployed
• Cough > 8 weeks
• X-ray cavity
Variable
Age group
15-19
20-29
30-39
40-49
50+
Sex
Female
Male
Occupation
Salaried
Self-employed
Student
Unemployed
Others
Cough
No cough
<2 weeks
2-7 weeks
>8 weeks
Smear grade
Few ~ 1+
2+
3+
Xray cavity
No
Yes
Confirmed TB
Total Case % 95% CI
p
OR
Odds Ratio
95% CI
p
210
464
314
214
224
5 2.33 (1.00-5.33) 0.001 **
19 3.93 (2.53-6.06)
28 8.19 (5.72-11.58)
14 6.14 (3.69-10.04)
5 2.18 (0.94-5.01)
1.00
1.75 (0.69-5.34) 0.272
4.01 (1.66-11.97) 0.005 **
2.87 (1.08-9.01) 0.047 *
0.94 (0.26-3.41) 0.918
669
751
38 5.37 (3.94-7.29) 0.275
33 4.21 (3.01-5.85)
1.00
0.76 (0.47-1.23) 0.268
375
167
265
372
247
15 3.85 (2.34-6.25) 0.167
8 4.57 (2.33-8.76)
10 3.64 (1.99-6.56)
28 7.00 (4.89-9.93)
10 3.89 (2.13-7.01)
1.00
1.21 (0.48-2.84)
0.94 (0.40-2.11)
1.95 (1.04-3.81)
1.01 (0.43-2.27)
170
155
655
444
3 1.73 (0.59-4.97) 0.078
5 3.12 (1.34-7.11)
35 5.07 (3.67-6.97)
28 5.93 (4.14-8.44)
1.00
1.86 (0.45-9.17) 0.403
3.14 (1.11-13.15) 0.060
3.75 (1.31-15.82) 0.032 *
790
299
337
31 3.78 (2.67-5.31) 0.111
19 5.97 (3.86-9.14)
21 5.87 (3.87-8.80)
1.00
1.66 (0.91-2.96) 0.090
1.63 (0.91-2.86) 0.094
959
467
40 4.00 (2.95-5.41) 0.051
31 6.22 (4.42-8.70)
1.00
1.63 (1.00-2.64) 0.046 *
0.674
0.884
0.042 *
0.976
POLICY IMPLICATIONS and
FUTURE DIRECTIONS
• Include active contact investigation in the national
guidelines
• Introduce new contact investigation form and use it by
health providers
• Involve primary health providers and social workers
• Consider to implement active contact investigation
• Strengthen collaboration between:
– Primary health care providers (Family group practice)
– District TB dispensaries
– Local governors’ office
ACKNOWLEDGEMENT
•
•
•
•
Dr Gantungalag, National TB Programme
Dr Nobuyuki Nishikiori, STB, WPRO
Dr Fukushi Morishita, STC
TB surveillance and research department,
NCCD
• District health departments in Ulaanbaatar
• TB doctors at the district TB dispensaries
• Primary health care providers (FGPs) in
selected districts
THANK YOU!