The Lower Leg
advertisement

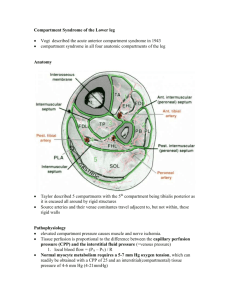
The Lower Leg ANATOMY Bones Tibia Fibula MUSCLES The muscles are in four compartments with 2-4 muscles in each compartment Compartments are held together by fascia MUSCLE COMPARTMENTS 1. 2. 3. 4. LATERAL – everts the ankle ANTERIOR – dorsiflexes the ankle DEEP POSTERIOR – plantarflexes the ankle (the calf muscle) POSTERIOR MEDIAL – inverts and plantarflexes the ankle Page 317 and 318 Major Muscles and Actions Anterior Tibialis - dorsiflexor Peroneals - evertors Gastrocnemius – plantarflexor Soleus – plantarflexor Posterior Tibialis – invertor INJURIES Muscle Cramps Sudden, violent contraction of the calf muscles Causes: Fatigue, overtraining, dehydration, poor nutrition, injury, poor flexibility – sharp pain in the calf, toe is pointed Tx: gentle stretch, ice, hydrate, can return to play if subsides and does not continue S/S: INJURIES STRESS FRACTURE Cause: Repetitive pounding with training S/S: Hurts more with and after activity, pain on one spot on bone Tx: Requires x-ray, possibly a bone scan If positive, no weight bearing for at least 2 weeks, no running for 4-6 weeks INJURIES MEDIAL ‘SHIN TIBIAL STRESS SYNDROME SPLINTS’ Occurs in distal 2/3 of posterior/medial tibia Causes: pronation, lack of flexibility in the lower legs, hard surfaces, hills, muscle weakness, poor shoes INJURIES MEDIAL S/S: TIBIAL STRESS SYNDROME resisted plantar flexion and inversion should hurt, pain is just off the tibia Treatment : prevention (shoes, arch support), strengthening, stretching, ice massage, contrast bath, tape arches Refer to MD if no improvement to rule out stress fracture INJURIES COMPARTMENT Occurs SYNDROME when pressure increases in compartment and shuts off blood and nerve supply to the foot Most often occurs in the anterior and deep posterior compartment THREE TYPES Acute Acute Exertional Chronic INJURIES ACUTE COMPARTMENT SYNDROME Medical emergency Causes: direct blow to the lower leg Usually in the anterior lower leg Symptoms come about several hours later S/S: compartment is tense, warm, red and shiny; complains of (c/o) deep aching pain; circulation and sensory problems in foot Tx: ice, elevation – refer to ER immediately INJURIES ACUTE EXERTIONAL/CHRONIC COMPARTMENT SYNDROME Cause: running and jumping activities S/S: With activity, foot goes to sleep, crampy pain, and tingling. When activity stops, it goes away. Consistent as to when it comes on with activity Tx: ice, activity modification, stretching, massage, and referral to the doctor (possible surgery) INJURIES ACHILLES Chronic, TENDINITIS overuse condition that comes about gradually Causes: running and jumping, repetitive stress, running up hills, poor flexibility S/S: achy type pain, Achilles is tender on palpation, pain with standing plantarflexion, may have crepitus, hurts to warm up and to cool down INJURIES ACHILLES TENDINITIS TREATMENT If there is crepitus, no running for 1-2 weeks Stretch! Heel lift in both shoes Orthodics Heat and/or ice INJURIES ACHILLES Achilles TENDON RUPTURE in largest tendon in body For Gastronemius and Soleus muscles Most common tearing spot is 1” above its insertion on the calcaneus Causes: Sudden, forceful plantar flexion and extension of the knee, age, previous tendinitis S/S: Feel and hear a snap, “kicked in the leg”, very weak plantarflexion, no Achilles observed Tx: Immobilization to ER, surgery? TEST FRIDAY, FEB 20th FOOT ANKLE LOWER LEG ANATOMY INJURIES Causes Signs and Symptoms Treatments