Care of Moderate and Severe Burns
advertisement

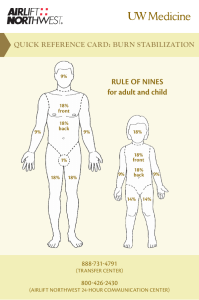
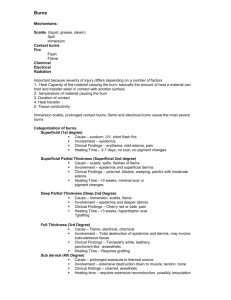
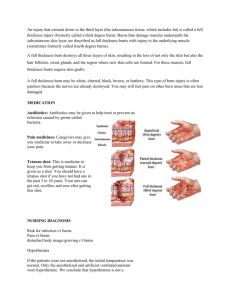
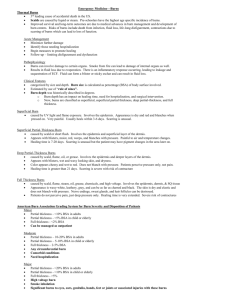
Pediatric Burns Carolyn O’Donnell, MD Epidemiology Worldwide: Young children- 60-80% scalds Older children- fire injury more likely >/= 5 yrs: 56% with flame burns Inflicted burns: usually scalds (stocking distribution typical), < 4 yrs of age Mortality related to size, depth, and presence of inhalational injury Symmetric Stocking Distribution Pathophysiology Thermal injury->protein denaturation and coagulation->irreversible tissue damage Surrounding zone of decreased perfusionpotentially salvageable Depth determined by intensity and duration of exposure Deeper Burns more common in young children with thinner skin Prolonged contact High heat High viscosity Systemic Response Damaged tissue ->vasoactive mediators (cytokines, prostaglandins, free radicals) Increased capillary permeability-> increased fluid in surrounding interstitial space Capillary leak: 18 to 24 hours Large burns: can see myocardial depression Major burns: hypotension, edema (burn shock, burn edema) Large Burns Can see myocardial depression Red Blood Cell destruction Local destruction of up to 15% of RBCs Decreased RBC survival time- can-> additional 25% reduction Metabolic Response Hypermetabolic response: Increased catecholamines, glucagon, cortisol -> increased metabolic rate, catabolism Decreased growth hormone, insulin-like growth factor (anabolic hormones) Classification Minor, moderate and major (ABA)- based on depth and size Treatment and prognosis based on classification Burn Size Accuracy is important- often underestimated Often determines management Typically expressed as percentage of total body surface area (TBSA) Lund and Browder chart useful Palm size- approximately 0.5% TBSA Burn Depth Can appear more superficial initially and progress Superficial- involve only the epidermal layer of skin Painful, dry, red, blanch with pressure Heal in 3-6 days No scarring Superficial Superficial Partial Thickness Epidermis and superficial dermis Painful, red, weeping, blanch with pressure Usually form blisters Heal in 7-21 days Scarring is unusual Can see pigment changes Superficial Partial Thickness Deep Partial thickness Extend to deeper dermis (hair follicles/glandualr tissue) Less painful than superficial partial Usually blister, wet or waxy dry Nonblanching Color variable- red to cheesy white >21 days to heal, scarring can be severe Can be hard to distinguish from full-thickness Deep Partial Thickness Full Thickness Extend through dermis Often painless Waxy white to leathery gray to charred and black Skin dry and inelastic, nonblanching Severe scarring- sometimes with contractures Full thickness Fourth degree Extend to underlying tissues like fascia, muscle Grading System Minor: <10% TBSA in adults, <5% in kids or older adults, <2% full thickness Moderate: 10-20% in adults, 5-10% young or old, 2-5% full thickness, high voltage injury, suspected inhalation injury, circumferential burn, underlying medical condition predisposing to infection Major >20% TBSA in adults, >10% young or old >5% full thickness High voltage burn Known inhalation injury Significant burn to face, eyes, ears, genitalia, or joints Significant associated injuries- fall, etc Pre-Hospital care ABC’s, supplemental oxygen Intubation if airway burn/inhalation Remove burned clothing and jewelry Cover area with clean sheet (warmth) Establish vascular access if possible- IV fluids, pain medications Cooling Immediate cooling can be beneficial Cool with water 10-20 minutes after burn Water temp no less than 8 Celsius No ice, no butter Watch for and take measures to prevent hypothermia ABC’s Airway: Look for signs of inhalation injurysoot in mouth, facial burns, stridor, hoarseness. Intubate early if concerned Breathing: Ventilation/oxygenation can be affected by toxins (CO), associated injuries, decreased level of consciousness, circumferential burns (chest/abdomen) Circulation: evaluate for associated injuries if VS changes, poor perfusion Examination Thorough general examination, obtain weight if possible Skin exam: Size and depth of burn Early eye exam including fluorescein stain to look for corneal burns Note external ear burns: risk for suppurative chondritis Circumferential burns- very close monitoring of distal perfusion/capillary refill (compartment syndrome), and respiratory status Diagnostic Studies Baseline CBC, electrolytes UA may reveal myoglobinuria if muscle injury Carbon monoxide levels Consider CXR, soft tissue neck films Others based on presentation Management Airway: Anticipate difficult airway Rapid sequence intubation: avoid BP lowering sedatives (etomidate okay), avoid succinylcholine if >48 hrs due to increased risk of hyperkalemia Monitor ETT closely- avoid accidental extubation Management Reliable IV access for fluid resuscitation Consider bladder catheter to reliably measure UOP Tetanus vaccine if >5 yrs since booster Tetanus immune globulin if incomplete primary immunization (less than 3) Consider surgical consultation IV Fluids Parkland formula: 4 ml/kg per %TBSA in 24 hours in addition to maintenance fluids Half of fluid given over 1st 8 hours, 2nd 50% given over the next 16 hours 4:2:1 for maintenance fluids/hour Ringer’s lactate often used (LR) in 1st 24 hours. D5LR often used for children <20kg Consider colloid/albumin after 24 hours to improve oncotic pressure Monitoring Very close Is/Os <30 kg: UOP 1-2ml/kg/hr >30 kg: 0.5-1 ml/kg/hr If increased UOP: check for glucose (osmotic diuresis) If decreased UOP: increase fluid, evaluate renal function Monitor HR and BP (pain may factor in) Can see metabolic acidosis w/ inadequate fluid resuscitation (also w/ CO, cyanide exposure) Pain control- morphine, fentanyl Wound Management Clean with mild soap and water Avoid disinfectants Remove clothing and debris Debridement of devitalized tissue with sterile saline soaked gauze Large, painful blisters and those likely to rupture should be removed Wound Dressing Topical antibiotic covered with nonadherent dressing, then covered with tubular net or gauze bandage Ideally: biologic dressing for deeper burns Topical Abx: Silver sulfadiazine 1%- broad antimicrobial, decreases pain, delayed healing Mafenide- penetrates well, broad spectrum, painful on application. Limited to cartilage, established infectionscan -> metabolic acidosis in large amount Bacitracin- often used on face- painless, doesn’t bleach pigment from skin Dressings should be changed frequently- 1-2x/day Escharotomy A consideration in partial and full thickness burns which can lead to functional impairment (often seen as edema increases) Involves incision completely through the depth of the burn eschar Can relieve restriction (chest burns) and reduce pressure (compartment syndrome) Escharotomy References Up to Date online Google images