Orthopedic Trauma
advertisement

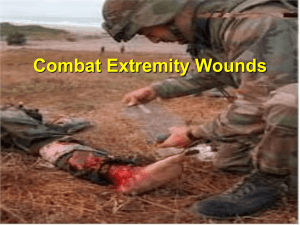
EXTREMITY INJURIES IN THE BATTLEFIELD CDR JOHN P WEI, USN MC MD 4th Medical Battallion, 4th MLG BSRF-12 Improved body armor has reduced axial trauma Skeletal trauma on battlefield has increased Severity of wounds and energy absorbed by injured limbs much greater INTRODUCTION Factors effecting extremity wounds Early management of extremity wounds Interventions for extremity wounds FACTORS IN EXTREMITY INJURIES FACTORS IN EXTREMITY INJURIES • • • • • Energy level (height of a fall / speed of car / caliber of bullet) Degree of contamination (soil, broken glass, shrapnel) Degree soft tissue injury (crushed / avulsed) Complexity of fracture pattern (number of bony pieces) Vascular injury HIGH ENERGY High-energy sources produce wounds characterized by violent tissue destruction Violent tissue destruction and contamination requires radical débridement of devitalized tissue FRACTURE TYPES COMPOUND FRACTURE Compound fractures (open fracture) : injury occurs with break in skin around broken bone Compound fractures require surgery to clean the site of injury and stabilize the fracture COMMINUTED COMPOUND FRACTURE COMPOUND FRACTURES AFTER IED BLAST MANAGEMENT OF EXTREMITY INJURIES •Initiate basics of trauma life support: airway, breathing, circulation •Assess for life threatening injuries •Control hemorrhage •Intubate for airway control if needed •Begin resuscitation •Secondary survey of extremities •Complete neurologic and vascular examination EXTREMITY INJURIES Concomittant vascular injuries require urgent surgical repair in addition to orthopedic fixation TRAUMATIC AMPUTATION attention must be focused on associated lifethreatening injuries commonly due to explosive munitions, with penetration and blast effects (parachute Injuries) COMPARTMENT SYNDROMES • Caused especially by crush injuries, electrical burns, circumferential scars, tight casts, hematoma in compartment, snake bites, and anything else that can increase pressure in a compartment • If untreated surgically, can lead to neurovascular compromise and ischemia resulting in gangrene COMPARTMENT SYNDROME Severe, constant pain in affected limb, pain on muscle palpation, passive stretch, and active contraction Paresthesia and loss of distal pulses are late signs and indicate poor outcome Can measure compartment pressures (if > 25 mm Hg) FASCIOTOMIES •Need to perform complete fasciotomy in all 4 compartments •All fascial envelopes opened completely from knee to ankle •Less frequently, fasciotomies of upper extremities, thighs, and buttocks are performed FIELD MANAGEMENT OF EXTREMITY WOUNDS • Control of hemorrhage • Temporary splinting • IV antibiotics • Tetanus prophylaxis COMBAT APPLICATION TOURNIQUET • • • One-handed application Tourniquet can be applied by soldier to himself if needed Controls hemorrhage from extremity wounds until evacuated to higher level of care IMMOBILIZATION OF EXTREMITY INJURIES • • • Essential to immobilize any fractures prior to CASVAC from field Failure to immobilize fractured extremities could lead to vascular or neurologic injuries or increased bleeding TREATMENT OF FRACTURES Débridement Reduction Fixation Evacuation WOUND MANAGEMENT FRACTURES AND WOUND MANAGEMENT • • • Treat by irrigation and debridement as soon as feasible to prevent infection Neurovascular status of the extremity should be documented and checked repeatedly Biplanar radiographs should be obtained PULSE LAVAGE High pressure irrigation can remove enough wound bacteria to render the wound noncontaminated but only if the irrigant is delivered with sufficiently high pressure ( <7 PSI) to mechanically remove bacteria from the wound surface ANTIBIOTIC BEADS AND SPACERS After fracture stabilization has been completed, bone defects may be filled with antibiotic-impregnated methacrylate beads. these beads provide local depot administration of antibiotic and maintain space for subsequent bone graft INTERNAL FIXATION OF FRACTURES • Internal fixation is the definitive treatment for compound fracture • This procedure is not performed in theater due to risk of contamination and infection EXTERNAL FIXATION OF FRACTURES EXTERNAL FIXATION OF FRACTURES • • • • Technically easier to perform in field conditions No soft tissue dissection or extended exposure required Ease of removing hardware Less risk of infection EXTERNAL FIXATION OF FRACTURES • • • Pin tract infections Delayed union Non union or mal-union AMPUTATION IN FIELD •Surgical preparation of the entire limb •Only amputate nonviable and ischemic tissue •Completion amputation through wound preferrable •Ligate major arteries and veins •Debride bony stumps •Dress wound in open manner with VAC dressing •Definitive revision of wound at later time SUMMARY • • • • • • • • Treatment of extremity injuries begins with ABC of trauma protocol Control hemorrhage Stabilize vital signs Evaluate neurologic and vascular status Stabilize fracture Debride wound Fasciotomy if indicated Casevac to next level of care