“Take a deep breath”
The Ageing Lung
Aylene Kelman
SpR
Consideration of age in lung
function
Everyone
needs to breathe!
Age related physiological changes in
the lung
Increased duration of exposure to
“lung insults”
Higher consequence on morbidity
and mortality
Ageing may influence response to,
and treatment, of lung disease
Physiology of the ageing lung
Limitation
of knowledge
Many respiratory studies don’t
include the older patient esp after
the age of 80
Is “ageing of the lung” intrinsic or
extrinsic?
Major changes in lung physiology
with age or “Intrinsic ageing”
Reduced
Lung elasticity
Respiratory muscle
strength
Chest wall compliance
FEV1 (declines before FVC)
Bronchial hyperresponsiveness
Perception of
bronchoconstriction
Diffusion capacity
Arterial oxygen pressure and
saturation
Ventilatory response to
hypoxia and (more
worryingly) hypercapnia
Increased
Residual volume
Lung compliance
Oxygen uptake on exercise
Unchanged
Total lung capacity
Airways resistance
Pulmonary arterial resistance
Arterial CO2 levels
The decline
“Extrinsic lung ageing” – factors identified in
age related decline of FEV1
Tobacco smoking
Occupational exposure
Asthma
Atopy
Obesity
Excessive alcohol consumption
Respiratory infection in early life
Nutritional status at birth
Maternal or passive smoking
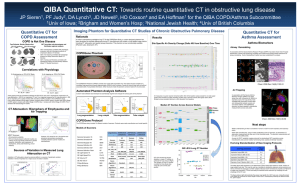
Lung Cancer
Figure 1.1: Numbers of new cases and age specific incidence rates,
by sex, lung cancer, UK 2003
Male cases
Female cases
Male rates
Female rates
Number of cases
4,000
400
3,000
2,000
200
1,000
Rate per 100,000 population
600
5,000
0
85+
80-84
75-79
70-74
65-69
60-64
55-59
50-54
45-49
40-44
35-39
30-34
25-29
20-24
15-19
10-14
5-9
0-4
0
Age at diagnosis
Most common cancer in the world today
2nd most common cancer diagnosis in UK, 1 in 7 of all cases
Incidence peaks between 70 and 79
Long smoking history is main factor for increasing incidence with age
Lung Cancer
Treatment led by the evidence base- but
studies of cancer treatment rarely include
the elderly
Many treatments contraindicated because
of co existing morbidity (chemotherapy
agents can be cardiotoxic and
nephrotoxic)
Several studies show that age is still a
major factor influencing treatment choice
Asthma and COPD
Asthma has been shown to be at least as
common in the elderly as in younger age
groups
In one study of 2000 subjects over 75,
28% had experienced wheeze in the last
12 months and 60% had had at least one
respiratory symptom
Diagnosis can be difficult
Incidence of COPD rises markedly with
increasing age
Asthma and COPD
Studies show that age alone does
not influence response to treatment
Factors which can influence
treatment include
Cognition
Side effects (esp steroids)
Compliance
Manual dexterity
Hindrance or help?
Respiratory infections
Incidence
of community acquired
pneumonia(CAP) substantially higher
in older people, especially men
60% of over 70’s hospitalised with
CAP will die
Age is a prognostic factor in severity
of CAP (CURB 65)
Most common pathogen is still
streptococcus pneumoniae
Respiratory infections – Hospital
acquired infection
Majority
of nosocomial infections
happen in over 65 age group
Significant proportion of these are
respiratory related
Over 60’s twice as likely to contract
hospital acquired pneumonia as
under 60’s
Often a terminal event for the frail
and elderly - “ the old man’s friend”
Respiratory Infections – other
considerations
Tuberculosis
Influenza
Aspiration
DONT
pneumonia
FORGET IMMUNISATION!
Any Questions?