Morbidity & Mortality: Esophagectomy
advertisement

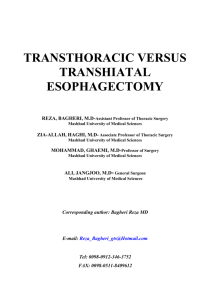
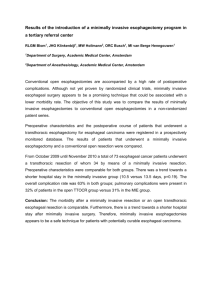
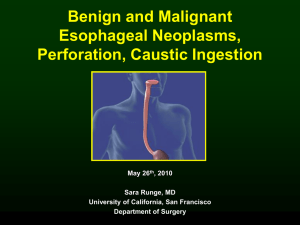
Diagnosis & Surgical Management of Esophageal Malignancies PETER J. DIPASCO, MD ASSISTANT PROFESSOR OF SURGERY DEPARTMENT OF SURGERY – SECTION OF SURGICAL ONCOLOGY THE UNIVERSITY OF KANSAS MEDICAL CENTER FRIDAY, APRIL 4TH, 2014 ACOS GENERAL SURGERY IN-DEPTH REVIEW Disclosure I have no disclosures Epidemiology Esophageal Adenocarcinoma Melanoma Prostate Others: Breast Lung, Colorectal Demographics In the United states 80+% of esophageal cancers are adenocarcinomas Over past 30 years: 400% increase in white males 300% increase in white females 100% increase in African-American males Male:Female ratio 7:1 Peak incidence 55 – 65 years old Risk Factors Molecular Biology Esophageal Cancer Work-up/Staging Endoscopic Ultrasound T – Stage N – Stage Formal CT scan and PET scan Metastatic disease Staging Updates Changes in new AJCC 7th addition Squamous Cell versus Adenocarcinoma Goal to remove 15 lymph nodes Esophageal Cancer Treatment Overview Proximal Definitive Chemoradiation therapy Metastatic Definitive Chemoradiaiton therapy No role for palliative resection HGD, T1, maybe T2 Primary Treatment is Surgical All others Multimodality approach Diagnostic Endoscopy Shortcomings: Currently low positive predictive values for Barrett’s esophagus diagnosis Possibly improved with magnification chromoendoscopy Only 5% of patients with Barrett’s esophagus progress to esophageal adenocarcinoma No data demonstrates that endoscopic surveillance decreases the incidence of advanced cancer and improves survival Alternative “Limited Approach” Treatments of Barrett’s High-Grade Dysplasia (and “Early” [mucosal] Adenocarcinoma) Rationale: Some “expert centers” claim highly accurate endoscopic detection Morbidity and mortality of esophagectomy continues to be high True high-grade dysplasia and early mucosal adenocarcinomas rarely metastasize to lymph nodes Limited Approach Endoscopic Ablation Two Categories Thermal Forms Photodynamic therapy Endoscopic Mucosal Resection (EMR) Combination Ablation / EMR Limited Resection Endoscopic Ablation Thermal Forms Multipolar coagulation Heat probe therapy Argon plasma coagulation Laser therapy (many types) Radiofrequency ablation Photodynamic Therapy Systemic photosensitizer Preferentially taken up by dysplastic tissue/tumor Expose tissue to light of specific wavelength Debride devitalized tissue Endoscopic Ablation Deficiencies No tissue removed to assure adequate targeting Islands of Barrett’s esophagus +/- cancer can still exist under ablated tissue Surveillance afterward difficult High stricture rates (30%) Endoscopic Mucosal Resection Technique Create pseudo polyp with epinephrine Snare Shortcomings Technically difficult Difficult to perform in long segment Barrett’s High recurrence rate (30%) May have diagnostic value Endoscopic Mucosal Resection Inject and Cut Inject, Lift, and Cut Inject, Suction, and Cut Ligate, then Snare Limited Resection Stein et al. J Surg Onc; 2005, 92:210-217 Methods of Esophagectomy Transhiatal Esophagectomy Transhiatal Esophagectomy Transhiatal Esophagectomy Transhiatal Esophagectomy Ivor-Lewis Esophagectomy Ivor-Lewis Esophagectomy Radical Lymphadenectomy vs. Limited No data supports a superiority of either approach Overall survival unchanged Latest NCCN guidelines rather identify a minimum number of nodes to obtain Morbidity & Mortality: Esophagectomy Hospital-Volume Outcome: Esophagectomy Metzger et al. Dis Esoph; 2004, 17:310-314 <5 5 - 10 11 - 20 > 20 Chemotherapy and Radiation Therapy for Esophageal Cancer Neoadjuvant Chemotherapy +/- Radiation Therapy Rationale Down-staging of tumor Increase “resectability” rate Improve the ability of surgeon to perform a complete (R0) oncologic resection Potentially prevent systemic spread at the earliest time-point of treatment Tumor “oxygenation” may be better prior to surgery, thus enhancing effectiveness Better compliance than if given post-operative Better assessment of biology of tumor 20% have complete pathologic response Recent data has shown a survival advantage Adjuvant Chemotherapy Large Randomized Prospective Studies (*versus Surgery Alone) No large randomized prospective studies performed for adenocarcinoma Possibly due to high morbidity and mortality of surgery – i.e. poor compliance Several advantages to neoadjuvant therapy Recent Meta-analyses show modest survival advantage Definitive ChemoRadiation Therapy Large Randomized Prospective Studies (***versus Surgery Alone) No study ever performed Recent studies show similar survival when compared to historical controls Indications Unresectable tumor or metastatic disease Medically unfit patient Cervical esophageal cancer Chemoradiation Therapy SUMMARY Resectable advanced non-metastatic dz Neoadjuvant Rx is standard of care Patients also receive post-op chemotherapy Regimens Paclitaxel and carboplatin Cisplatin and infusional 5-FU Current trends • Substitute oxaliplatin for Cisplatin • Substitute capecitabine for 5-FU Metastatic or Unresectable dz Triple “definitive” therapy Docetaxel + cisplatin and 5-FU or Epirubicin + platinum + 5-FU Can substitute utilizing oxaliplatin and capecitabine Add anti-HER-2 therapy when appropriate 30% of patients Palliative Therapy Epidemiology >50% patients are inoperable due to: Unresectable tumor Metastatic disease Poor medical condition Goal Relieve dysphagia rapidly with no hospital stay Basic principles Currently, no indication for “palliative esophagectomy” Treatment should be individualized Wide range of options CASE STUDY 55M with daily sx’s of reflux for 15yrs 15lb unintentional weight loss x2mos PCP orders esophagram – distal mucosal irregularity – refers to you Diagnostic tests? Imaging? Staging? Surgical Plan?