Diagnostic and Maintanence Tools
advertisement

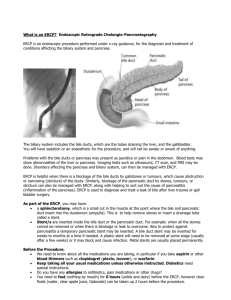
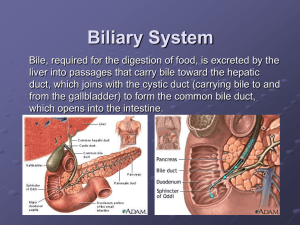
Pancreatic Cancer: Diagnostic & Maintenance Tools Felice Schnoll-Sussman, MD Jay Monahan Center for Gastrointestinal Health New York Hospital/ Weill Cornell Medical College Normal Hepatobiliary Anatomy An abnormality of the hepatobiliary system is suspected... WHAT IS THE NEXT STEP??? ULTRASOUND CT SCAN MRCP ??? MRI EUS CA19-9 Ultrasound Least invasive radiologic technique Portable, quick and can guide interventional procedures No ionizing radiation High sensitivity for detected dilated bile ducts and biliary tract obstruction (obstructive jaundice) Very sensitive for differentiating cystic from solid lesions Overlying gas may obscure visualization Ultrasound (Sonogram) Patient Preparation Clear liquid diet for 24 hours prior to exam Liquids include clear juices such as apple, cranberry & grape, clear soups, jello, coffee or tea. No milk products or carbonated bevarages CT SCAN (Computed Tomography) Primary imaging study for patients suspected of having pancreatic lesion Thin section dual-phase spiral CT scan Obtained during optimal pancreatic arterial and portal venous enhancement and hepatic phase CT (CAT SCAN) Patient Preparation Clear liquid diet for 24 hours prior to exam Patients with prior reactions to iodinated contrast or allergic history require pretreatment medication Diabetics: Alert doctor if your are taking glucophage ERCP (Endoscopic Retrograde Cholangiopancreatography) Patient Preparation Nothing by mouth after midnight the evening before procedure No aspirin or nonsteroidal medications one week before procedure Pancreatic Cancer ERCP Tools Sphincterotome ERCP Tools Balloon ERCP Tools Stents ERCP Tools Wallstent Normal ERCP Cystic Duct Bile Duct GB Pancreatic Duct Pancreatic Cancer stricture Balloon Dilatation of Stricture Diagnostic ERCP Double duct sign CBD Stricture Main PD stricture Stent Combined Procedure PTC ERCP Wall Street Journal October 28, 1981 MRI has arrived ... What is MRCP? Magnetic Resonance Cholangiopancreatography Well established tool for evaluating the biliary tree, pancreatic ducts and gallbladder Well tolerated Role: – To DIAGNOSE (not treat) diseases of the biliary and pancreatic ducts – To avoid invasive procedure risks – Reduce morbidity MRCP: Background MRI of the bile ducts and pancreatic ducts Relies on radiofrequency, pulse-induced excitation of protons within a magnetic field to generate an image Fluid in the biliary and pancreatic ducts serves as an intrinsic contrast medium The ductal systems appear white against the black background, providing images similar to those of ERCP MRI Patient preparation Inform doctor if you have any of the following: Surgical vascular clips Neurostimulators Cochlear Implants Breast Tissue Expander History of claustrophobia IVC Filter Penile Implants Pacemaker Silver backed dermal patches MRI Patient Preparation Do not wear make-up Music is available during the examination. Most centers will allow you to bring your own tape or CD Pancreatic cancer - ERCP vs. MRCP EUS ENDOSCOPIC ULTRASOUND EUS TOOLS EUS TOOLS EUS TOOLS Doppler Vessel Identification EUS (Endoscopic Ultrasound) Patient Preparation Nothing by mouth after midnight the evening before procedure No aspirin or nonsteroidal medications one week before procedure Pancreatic Cancer Staging Primary Tumor (T) TX Primary Tumor cannot be assessed T0 No evidence of primary tumor Tis Carcinoma in situ T1 Tumor limited to pancreas, 2 cm or less T2 Tumor limited to pancreas, greater than 2 cm T3 Tumor extends beyond pancreas, no celiac or SMA involvement T4 Tumor involves celiac axis or SMA (unresectable primary) Regional Lymph Nodes (N) NX Regional lymph nodes cannot be assessed N0 No regional lymph nodes N1 Regional lymph node metastasis Distant Metastasis (M) MX Presence of distant metastasis cannot be assessed M0 No distant metastasis M1 Distant metastasis CA 19-9 Tumor marker Amongst markers found to have the greatest sensitivity (70%) and tumor specificity (87%) Cutoff value of 70 U/ml Can be elevated with biliary tract obstruction by a noncancerous lesion The diagnosis is made... Can you do anything for the pain? Therapeutic EUS Celiac Plexus Block Conclusions Myriad of well established tools to help guide diagnosis and management Studies are complementary and should be used together Future holds great promise for additional innovations