Case Presentation - Abhilash Sailendra
advertisement

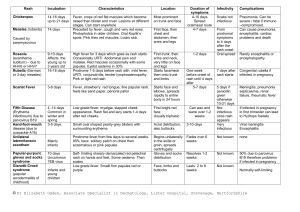
CASE PRESENTATION Abhilash Sailendra GPST 1 AN 18 MONTH OLD WITH FEVER AND RASH High fever for 4 days. Four days prior to admission , she developed high fever and rhinorrhea. She was taken to see a doctor at a clinic and was diagnosed as "URTI". She was prescribed paracetamol, and amoxicillin . Two days ago, she had semi-solid stool. One day PTA, she developed maculopapular rash at trunk at extremities. PMH : Healthy child . Birth weight was 3.0 kgs. No previous admissions to hospital. PHYSICAL EXAMINATION Fully conscious but irritable. Vital signs: Temp 39.8 C, HR 160 beats/min, RR 40 breaths/min, BP 98/50 mmHg Head to Toe : mild injected conjunctiva, no icteric sclera, red lips , normal anterior fontanel. No palpable LNs. Heart: regular rhythm, tachycardia Lung: clear, no added sounds Abdomen: soft, no organomegaly Skin : Erythematous rash at trunk and extremities , Extremities: Swelling of dorsal part of hands and feet Investigations: FBC: Hb 10.6 gm%, WBC 14 (N 72%,L 28%), platelets 324 U & Es - NAD URINE: Clear ESR - 97 mm CRP – 276 ECG: sinus tachycardia , rate 170/min, no ST-T change Echocardiogram: No structural heart defect, normal left ventricular function (EF 67%), minimal pericardial effusion 5mm. DIAGNOSIS ?? KAWASAKI DISEASE Syn - Kawasaki's syndrome, mucocutaneous lymph node syndrome, infantile polyarteritis nodosa. Course in the hospital : , She was given a high dose intravenous immunoglobulin (IVIG) 2g/kg and High dose oral aspirin ( 80mg/kg/day). Four hours after IVIG the fever dramatically subsided. Two days after IVIG ,her irritability, erythematous rash, red lip and oedema of extremities disappeared. She was discharged home with low dose aspirin (5mg/kg /day). Cardiology follow up in 6 weeks time. FEW FACTS Age group – 6 months to 5 years. Commonest cause of acquired heart disease in UK. Mortality in UK – 3.7 % Systemic Vasculitis Most important complication – Coronary Aneurysms ( 30 % ), and if treated early these could be avoided. DAIGNOSTIC CRITERION Along with fever > 38.5 , there must be at least four of the following to fit the diagnostic criteria (or echocardiographic evidence of coronary artery aneurysms): Inflammation and irritation of the lips, mouth and/or tongue Erythema, oedema and/or desquamation of the extremities Bilateral dry conjunctivitis Widespread non-vesicular rash Cervical lymphadenopathy >1.5 cm in size Classical features of Kawasaki disease Fever lasting ≥5 days Marked irritability of the child Erythema, swelling and desquamation affecting the skin of the extremities Bilateral conjunctivitis Rash Inflammation of the lips, mouth and/or tongue Cervical lymphadenopathy ATYPICAL SYMPTOMS Other possible features include lethargy, symptoms of urethritis, diarrhoea, vomiting, abdominal pain, myalgia, arthralgia and arthritis. A recent Chinese survey found that there appears to be an appreciable incidence of atypical or 'incomplete' Kawasaki disease and that such cases appear to have a high prevalence of coronary artery lesions. The presence of peri-anal desquamation may be a useful indicator of the likelihood of such 'incomplete' cases An 8 year old child presents with his parents to his Physician. His chief complaint is a rash that began on his lower extremities a few hours ago. In addition his parents state that the kid has had a low grade fever, arthritis and colicky abdominal pain. A purpuric rash limited to the lower extremities was found on examination. A urinalysis reveals RBC casts and mild proteinuria. The platelet count is normal. The mostly diagnosis is – A . Systemic Lupus Erythematosis ( SLE ) B . Rocky mountain Spotted fever C . Idiopathic Thrombocytopaenic Purpura ( ITP ) D . Henoch – Schonlein Vasculitis E . Post Streptococcal GN A 6 year old girl who appears healthy is brought to the GP by her mother because of a rash. The mother states that the child had been well until 2 days ago, when she developed fever and upper respiratory tract symptoms. Yesterday the child had erythematous facial flushing that spread as a macular red lesion to her proximal extremities and trunk, which now has a lacy appearance. The most likely diagnosis is – A . Erythema Infectiosum B . Roseola C . German Measles or Rubella D . Measles E . Scarlet Fever A 4 year old presents with a temperature of 40 C, which she has had for the last 4 days. Her GP had seen her on the first and 3rd day of fever. He was unable to ascertain the source of fever, and reassured the mother with Calpol and Ibuprofen. He now presents to AED. On examination the child is noted to have conjunctivitis, erythematous rash, cervical adenopathy and swollen hands and feet. Lab findings show neutrophilic leukocytosis, elevated ESR and normal platelets. The most likely diagnosis is – A . Scarlet Fever B . Acute Rheumatic fever C . Juvenile Rheumatoid Arthritis D . Toxic Shock Syndrome E . Kawasaki Disease A 4 year old boy presents with fever and conjunctivitis. The mother states that the child had been in good health until 2 days ago when he developed URTI symptoms. She also mentions that he has photophobia and cervical adenopathy. On examination red lesions with a white centre are present on the buccal mucosa. A generalised blanching erythematous rash is also noted . The most likely diagnosis is – A . Kawasaki Disease B . Rubella C . Adenovirus infection D . Measles E . Still s Disease TAKE HOME MESSAGES 1 . In a child with a fever you should always consider conditions with a higher risk of serious outcomes, including: Meningitis Pneumonia Urinary tract infection Septic arthritis/osteomyelitis Herpes simplex encephalitis Kawasaki disease 2. Any febrile child with purpuric rash is considered as Meningococcal Septicaemia unless proved otherwise. CRASH AND BURN CONJUNCTIVITIS RASH ADENOPATHY STRAWBERRY TONGUE HANDS AND FEET – RED SWOLLEN FLAKY SKIN BURN – FEVER > 40 FOR > 5 DAYS Thank you for your patience….



![Mistry-VisualDiagnosis12-5-07[2]](http://s2.studylib.net/store/data/005753399_1-f3c8e8f06b6b9b9f31dbd547ba21de96-300x300.png)