Capsule Endoscopy in Tamworth
advertisement

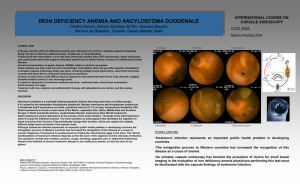
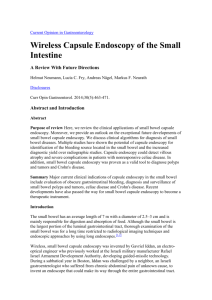
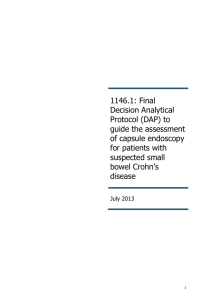
Capsule Endoscopy in Tamworth True or False: “Capsule Endoscopy is a useful test in the diagnosis of unexplained anaemia” FALSE Importance of Pre Test Probability MBS – Item Number 11820 obscure gastrointestinal bleeding, using a capsule endoscopy device approved by the Therapeutic Goods Administration (including administration of the capsule, imaging, image reading and interpretation, and all attendances for providing the service on the day the capsule is administered), (not being a service associated with double balloon enteroscopy), if: (a) the service is performed by a specialist or consultant physician with endoscopic training that is recognised by The Conjoint Committee for the Recognition of Training in Gastrointestinal Endoscopy; and (b) the patient to whom the service is provided: (i) is aged 10 years or over; and (ii) has recurrent or persistent bleeding; and (iii) is anaemic or has active bleeding; and (c) an upper gastrointestinal endoscopy and a colonoscopy have been performed on the patient and have not identified the cause of the bleeding; and (d) the service is performed within 6 months of the upper gastrointestinal endoscopy and colonoscopy Understanding the “O’s” of GI Bleeding Obscure Cause not identified Inpractice, obscureafter GI endoscopies bleeding is either (up to10% - 75% will be due to small bowel lesions) overt or causes iron deficiency Overt Melaena or haematochezia Occult Not Overt Diagnosing Iron Deficiency Iron Deficiency ↓ Systemic Disease ↓ Mixed Transferrin ↑ ↓ ↓ Transferrin Saturation Ferritin ↓↓ ↓/N/↑ ↓ ↓ ↑ ↓/N/↑ Transferrin Receptor ↑ N ↑ Iron ↓ Initial Iron Deficiency Workup Consider ExtraIntestinal Causes Dietary Pregnancy, Lactation Menstruation Haemolysis Blood donation Haematuria Initial Iron Deficiency Workup Consider ExtraIntestinal Causes Gastroscopy Ulcers, Malignancy, Angioectasia, GAVE H. Pylori status Duodenal biopsies for coeliac disease Colonoscopy Malignancy, colitis, angioectasia, proctitis Include ileoscopy Good bowel preparation important Initial Iron Deficiency Workup If Endoscopies are non-diagnostic: Reconsider extraintestinal causes Consider Urinalysis and Coeliac disease serology Iron Replacement OR Early Capsule Endoscopy Iron Replacement OR Early Capsule Endoscopy Iron Replacement Early Capsule Endoscopy Younger Premenopausal Asymptomatic Never overt bleeding Observe for at least 3 months then recheck Hb and ferritin. If “recurrent or persistent bleeding”, then capsule endoscopy Older Male Symptoms, Weight loss Any overt bleeding Need to demonstrate “recurrent or persistent bleeding” – eg 2 low Hb’s, a positive FOBT after endoscopies etc Capsule Endoscopy Preparation Similar to colonoscopy Stop iron tablets 5 days prior Clear fluids afternoon before 2 sachets of PicoPrep 10 hour fast On the day Metoclopramide and simethicone What Does Capsule Endoscopy Visualize in the Small Bowel? Melanoma Overt bleeding Angioectasia Mass/tumor Inflammation by infection (eg, CMV) Ulcerated stenosis caused by NSAID use Inflammatory stenosis Bleeding ulcer Yield of Capsule Endoscopy 38 – 83% Depends largely on pre test probability Of small bowel lesions found: 60% angioectasia 30% ulcers / erosions 10% tumours Other Diagnostic Options Method Standard Radiological Imaging Bleeding Scan Diagnostic Yield • Low: 5% (unable to diagnose most vascular lesions) • Low: ~25% • Location accuracy: ~30–50% Angiography Double-Balloon Enteroscopy • Low: 25%–30% • 60%–80% Considerations • Impact on management: <10% •Useful for clinical suspicion of small bowel obstruction, tumors • • • • Sensitivity threshold: 0.3 mL/min Prerequisite to angiography Time-consuming Little or no benefit in typical OGIB • Sensitivity threshold: 0.5 mL/h • Invasive • Identifies bleeding/non-bleeding lesions • Time-consuming • Requires extensive training; additional nursing staff, anesthesiological support often required • Optimal patient selection required Diagnostic Options (continued) Method Diagnostic Yield Considerations Intraoperative Enteroscopy • 70%–100% • • • • • CT Enterography • Low: vascular • ~20% of submucosal lesions missed Transfusion-dependent (severe blood loss) Risk of continued bleeding (outweighs risk of therapy) Technically difficult Adhesions, luminal blood, infiltrating neoplasia Complications (during and after procedure) malformations, ulcerative disease Push Enteroscopy • 15%–35% average • Variable for overt • May detect missed proximal lesions • Provides opportunity to identify and treat active bleeding and AVMs: 5%–65% Small Bowel CE • 38%–83% bleeding (AVMs only) 25%– 85% of the time within a single year • Affects change in management in ≥87% of patients • (50%–66% remain transfusion-free) Low re-bleeding rates in patients with negative findings of CE (5.6%–11%) Complications Of Capsule Endoscopy Failure to enter the small bowel Failure to visualise all small bowel Dyspahgia, Gastroparesis Can insert endoscopically 10-16% Diabetics Capsule Retention <1% for OGIB, up to 10% for Crohn’s disease Caution with previous small bowel surgery or abdominal radiotherapy or clinical suspicion of obstruction DBE or surgery to remove capsule +/- resect lesion What to do with the Result Negative : Observe unless symptoms suggest further investigation Tumours : Consider resection Ulcers : Stop aspirin/NSAIDs, consider Crohn’s disease Angioectasia : Reassurance and Iron Replacement (safest) Assess antiplatelet agents or anticoagulants If not controlled with iron, or intolerant of iron, then consider ablative therapy Via Gastroscopy, Enteroscopy or Colonoscopy Patient Histology Capsule Endoscopy Quartile Surgical Quartile 1 Carcinoid 4 4 2 Adenocarcinoma 4 4 3 Adenocarcinoma 1 1 4 Gastrointestinal Stromal Tumour 3 2 5 Adenocarcinoma 1 1 6 Cavernous Haemangioma 2 3 7 Lymphoma 1 1 8 Gastrointestinal Stromal Tumour 3 2 9 Adenocarcinoma 4 4 10 Gastrointestinal Stromal Tumour 2 1 11 Hyperplastic polyp 1 1 12 Cavernous Haemangioma 3 2 13 Ectopic Pancreas 3 2 Identical quartile in 7/13 Different quartile by one in 6/13 350 Anterograde Push Enteroscopy 324 300 250 Angioectasia Number 200 164 Red Spot Ulcer 150 Tumour 105 104 100 58 57 57 47 50 28 16 10 5 15 2 2 1 0 1 3 2 Quartile 4 Other indications for Small Bowel Capsule Endoscopy Peutz-Jager syndrome Crohn’s disease* Coeliac disease* Abnormal SB radiology* * Not medicare rebateable Other Types of Capsules Patency Capsule Oesophageal Capsule Colonic capsule So how do I get one? Refer for a consultation OR Fax information across and I can have a look OR Refer directly yourself Questions?