Knee Evaluation knee_evaluation
advertisement

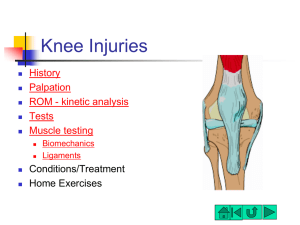
KNEE EVALUATIONS Quick Facts Patellofemoral Joint (PFJ) Variations in PFJ loading during OKC and CKC activities PFJ loading increases: – with increased flexion in CKC – with increased extension in OKC PFJ Loading Walking – 0.3 x body weight Ascending Stairs – 2.5 x body weight Descending Stairs – 3.5 x body weight Squatting – 7 x body weight History MOI - – Position of lower extremity at time of injury extended) (?foot planted, knee Previous history Pain (levels, types, descriptors) Unusual sounds/sensations “pop, clicking, snapping” Chronic vs. acute Location of pain “inside the knee” Surface Shoes Type of activity at time of injury Painful to walk up/down stairs; any clicking, catching Did it swell immediately, slowly? Is the swelling located in the knee or in a pocket? Observation Bilateral comparison Gait (limp, walking on toes, do they not want to extend knee, do they keep the knee stiff) Swelling (girth measurements) Discoloration Deformity (squinting patellae, “Frog-eyed” patellae, Patella alta, Patella baja) Genu valgum, genu varum, recurvatum Musculature – defined/mushy Q-angle The quadriceps angle (Q-angle) is the angle formed between a line drawn through the tibial tuberosity and the center of the patella and another line drawn from the anterior superior iliac spine (ASIS) of the pelvis through the center of the patella. Q-angle Knee in extension – Normal males: 13 degrees – Normal females: 18 degrees Knee in 90 degrees flexion – Both genders: 8 degrees Structural Alignment Genu Varum (Bowlegged) Genu Valgum (knock kneed) Boney Palpation Tibia – Tibial tuberosity – Tibial Condyles (medial + lateral) Pes Anserine Hamstrings – Semitendinosus tendon – Semimebranosus – Biceps femoris tendon Fibula – Head Medial joint line Medial collateral ligament Lateral joint line Lateral Collateral Ligament “Windows” Medial & Lateral Femoral Epicondyles Quadriceps muscle group – – – – Rectus Femoris Vastus Lateralis Vastus Intermedius Vastus Medialis Oblique Biceps femoris tendon Iliotibial band Popliteal fossa Gastrocnemius heads Patella Patellar tendon Boney Palpation Tibia – Tibial tuberosity – Tibial Condyles (medial + lateral) Fibula – Head Medial & Lateral Femoral Epicondyles Patella Surface Anatomy Patella (A) Femur (B) Tibia (C,E – tuberosity) Joint Line (D) Fibula (F) Boney Anatomy Bony Anatomy – Lower Leg Tibia – Bears most of the weight Fibula – Attachment place for muscles & ligaments – Upper Leg Femur – Patella Patella Sesamoid bone Imbedded in quadriceps & patella tendon Serves similar to a pulley for improving angle of pull (results in greater mechanical advantage in knee extension) Tendons + Ligaments Medial joint line Medial collateral ligament Lateral joint line Lateral Collateral Ligament “Windows” Pes Anserine – Semitendinosus tendon – Gracilis tendon – Sartorius tendon Semimebranosus tendon Biceps femoris tendon Quadriceps Tendon Biceps femoris tendon Iliotibial band Patellar tendon Internal Knee Anatomy Internal Knee Anatomy Medial Meniscus Lateral Meniscus Anterior Cruciate Ligament Posterior Cruciate Ligament Articular Cartilage Menisci Bursae & Fat Pad of the Knee Cruciate Ligament Movement Anatomy – Soft Tissue Quadriceps – – – – – Rectus femoris Vastus lateralis Vastus intermedius Vastus medialis oblique Hamstrings – – Biceps femoris – Semitendinosus – Semimembranosus Popliteus – Popliteal fossa Gastrocnemius + Soleus Tibialis Anterior Muscles Quick Facts Tibiofemoral Joint (TFJ) Normal ROM – Flexion 135-140 degrees – Extension 0 degrees Closed Pack Position – Full extension with ER Loose Packed Position – 25 degrees of flexion Knee Movements Screw Home Mechanism Locking mechanism as the knee nears its final extension degrees – Automatic rotation of the tibia externally (approx. 10 degrees) during the last 20 degrees of knee extension Femoral condyles are a different size – Medial has larger surface area The tibia glides anteriorly on the femur. As knee extends, the lateral femoral condyle expends its articular distance. The medial articulation continues to glide, resulting in external rotation of the tibia utilizing the lateral meniscus as the pivot point. ACL & PCL are rotary guides Special Tests Myotomes and Dermatomes Valgus Stress test Varus Stress Test Tinel Test Apley McMurray Anterior Drawer Lachmans Posterior Drawer Godfrey’s 90/90 Posterior Sag Patellar Apprehension Test Clark’s Sign Stress/Special Tests Check for swelling Check ROM Check integrity of ligaments & joint stability – Valgus, Varus, Lachman’s, Anterior/Posterior Drawer, Godfrey’s 90-90 Test/Posterior Sag Test, Check integrity of meniscus – McMurray’s, Apley’s Compression/Distraction, Duck Walk, Check integrity of patella – Patellar Apprehension, Q Angle, Clarke’s Sign, Special Tests Anatomy of the ACL 3 strands Anterior medial tibia to posterior lateral femur Prevent anterior tibial displacement on femur Secondarily, prevents hyperextension, varus & valgus stresses Biomechanics of the ACL Most injuries occur in Closed Kinetic Chain Least stress on ACL between 30-60 degrees of flexion Anteromedial bundle tight in flexion & extension Posterior lateral bundle tight only in extension ACL Tears Most common mechanisms – Contact: CKC with foot ER w/ valgus stress Hyperextension direct hit on the posterior tibia – Non-Contact: Most common Due to sudden deceleration Sudden landing, cutting, or pivoting Patient will c/o “buckling” or “giving away”, typically will hear and/or feel a “pop” Diagnostic Imaging Why perform an MRI after ACL injury? Anterior Lachmans Position: – Supine – Knee flexed to 20 – 30 degrees – Proximal hand on Femur above the patella, distal hand on Tibia just below Tibial Tuberosity Action: – Apply anterior force to the tibia with the distal hand while stabilizing the femur with the proxmial hand Positive Findings: – Anterior Cruciate Ligament Sprain Joint opening up Anterior Drawer Position: Action: – Hip flexed to 45o; knee flexed @ 90o – Foot on table in neutral – Examiner sits on foot w/ B hands behind the subject’s proximal tibia and thumbs on the tibial plateau – Apply anterior force to the proximal tibia, feeling the hamstrings for tightness Positive Findings – Anterior Tibial Displacement – Anterior Cruciate Ligament Sprain PCL Biomechanics Functions: – Primary stabilizer of the knee against posterior movement of the tibia on the femur – Prevents flexion, extension, and hyperextension Taut at 30 degrees of flexion – posterior lateral fibers loose in early flexion Posterior Cruciate Ligament Two bundles – Anterolateral, taut in flexion – Posteromedial, taut in extension Orientation prevents posterior motion of tibia PCL larger & stronger than ACL – CSA 120-150% larger – CSA AL 2x PM Consider associated role of posterolateral complex when discussing PCL – – – – LCL Popliteus Complex Arcuate Ligament Posterior Lateral Capsule PCL Injuries Very rare in athletics, usually due to MVA – Due to hyperextension, hyperflexion, or the tibia being forced posteriorly on the femur – Only 33% related to sports Isolated PCL Injuries unusual – Assess other ligaments Avulsion Injuries Mid-Substance Tears Posterior Drawer Test Position: – Hip flexed to 45o; knee flexed @ 90o – Foot on table in neutral – Examiner sits on foot w/ B hands behind the subject’s proximal tibia and thumbs on the tibial plateau Action: – Apply posterior force to the proximal tibia Positive Findings – Posterior Tibial Displacement – Posterior Cruciate Ligament Sprain Godfrey’s 90/90Test Position: – Hip flexed to 90o; knee flexed @ 90o – Examiner holds onto both heels Action: – Look for posterior translation of the tibia Positive Findings – Displacement of the Tibia – Posterior Cruciate Ligament Sprain Posterior Sag Test Position: – Lie on table Knee flexed to 90o; Hip flexion 45o Action: – Subject actively flexes Quads while hip remains in 45o – Look for a posterior translation of the Tibia in relation to the Femur Positive findings: – Posterior Cruciate Ligament Sprain MCL Biomechanics Primary role is to prevent against a valgus force and external rotation of the tibia Throughout Full Range of Motion: – Both fibers are taut in full extension – Anterior fibers are taut in flexion – Posterior fibers are taut in mid range MCL Sprains Typically due to valgus forces in CKC – Foot typically in neutral or externally rotated Most frequently injured ligament in the knee Usually no joint effusion unless deep portion affected since primarily located outside the joint capsule Valgus Stress Test Position: – Knee @ 0o and knee @ 30o – Proximal hand on Lateral joint line – Distal hand on the lower leg Action: – Apply medial force to lateral joint line; and lateral force to distal tibia Positive Findings – Medial Collateral Ligament Sprain LCL Biomechanics Primary role is to protect from varus forces and external rotation of the tibia, assists in 2° restraint for anterior and posterior tibial translation Throughout Range of motion: – Is taut during extension – Loose during flexion Especially after 30° of flexion LCL Sprains Typically due to varus forces, especially in CKC position with leg adducted and tibia internally rotated Usually occur during contact sports Typically has limited joint effusion since it is located outside of the joint capsule Varus Stress Test Position: – Knee @ 0o and knee @ 30o – Medial hand on Medial joint line Action: – Apply lateral force to medial joint line; and medial force to distal tibia Positive Findings – Lateral Collateral Ligament Sprain Meniscal Functions Deepens the articulation and fills the gaps that normally occur during the knee’s articulation Primary Functions – Load distribution – Joint Stability – Shock Absorption Secondary Functions – Joint Lubrication – Articular Cartilage Nutrition – Proprioceptive Feedback Mechanism of Injury Trauma – – – – Compression Rotational Force Valgus Force Usually Combination of Forces Degenerative Changes – Greater than 30 years old – No PMHX required – Often due to MOI that “seemed harmless” at time Noyes, 2002 states 60% of meniscal injuries associated with ACL injury Apley Compression – Position: Prone Knee flexed to 90o ; foot dorsiflexed – Action: Stabilize the femur with examiner’s knee Push down on ankle/lower leg and rotate – Positive findings: Pain = Meniscus No Pain = Ligament involvement Distraction – Position: Prone Knee flexed to 90o ; foot dorsiflexed – Action: Stabilize the femur with examiner’s knee Pull up on ankle/lower leg and rotate – Positive findings: No pain = Meniscus Pain = Ligament involvement McMurray Position: – Supine – Examiner’s standing with distal hand grasping the subject’s heel; proximal hand on subject’s knee with fingers palpating the medial and lateral joint lines Action: – Knee fully flexed, externally rotate the tibia and introduce a valgus force and extend the knee Medial Meniscus – Repeat with internal rotation of the tibia and Varus force. Lateral Meniscus Positive Findings: – “Clicking” indicates a Meniscal Tear Medial side = medial meniscus Lateral side = lateral meniscus Unhappy Triad MCL, ACL, Medial Meniscus Typically due to a valgus force with the foot planted PFJ Biomechanics During extension, patella glides cranially During flexion, patella glides caudally Patellar compression – OKC greatest at end range (final 30 degrees) – increases in CKC after 30 degrees of flexion Patellofemoral Pain Syndrome General term to describe anterior knee pain Caused by a variety of factors: Signs & Symptoms: – Poorly localized Pain – Little to no swelling – Pt. Tenderness under lateral patella – Insidious onset Clark’s Sign (Patellar Grind Test) Position: – Patient is lying supine w/ knee extended – Examiner places the web space of the thumb on the superior border of the patella Action: – Subject contracts the Quads while the examiner applies downward and inferior pressure to the patella Positive Finding: – Pain with movement of patella or inability to complete test – Chondromalacia patella or patellar femoral syndrome Patellar Apprehensive Test Position: – Patient is supine and relaxed Action: – Examiner grabs patella and pushes it in all 4 ways Superior / Inferior Lateral / Medial Positive Findings: – Patient Apprehension – Excessive Movement in one direction – Dislocating Patella Osgood-Schlatter’s Disease Housemaid’s knee