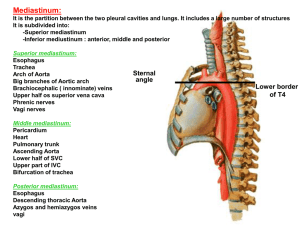
Basic Cardiovascular System and Pathological Abnormalities
advertisement

Approach to Common Cardiac Emergencies Agustin E. Rubio, MD Sibley Heart Center Cardiology Children’s Healthcare of Atlanta Emory School of Medicine Topics • Cyanosis & Ductal Dependent • Emergency Room Diagnoses: Tetralogy of Fallot Hypoplastic Left Heart Syndrome Coarctation of Aorta SVT • Shunt Dependent vs Non-shunt Dependent 2 Epidemiology Cardiac malformations • 10% of infant mortality Incidence: • 4-6/1000 live births Most common lethal diagnosis: • Left ventricular outflow tract obstruction Hypoplastic left heart syndrome Coarctation of aorta Aortic stenosis 3 Circulatory Transitions Conversion from right sided (placental oxygenation) to left sided circulation (pulmonary oxygenation) Progression is secondary: • Decreasing PVR • Closure of ductal shunts Clinical presentations: • Cyanosis • Respiratory failure • Shock 4 Cyanosis Typically, 2 g/dL of reduced hemoglobin • 5g/dL of reduced Hb clinical cyanosis Hb 15 cyanosis at 75-80% Hb 20 cyanosis at 80-85% Hb 6 cyanosis at 45-50% 5 Ductal Dependent Lesions Cyanosis CHF/Shock Rt to Lt shunting: Lt Ventricular Outflow Tract Obstruction: Tricuspid atresia TOF/ Pulm atresia Ebstein’s anomaly HLHS Coarctation of Aorta/ AS Truncus arteriosus TGA with VSD 6 TAPVR Left Ventricular Outflow Tract Obstruction Major source of neonatal M&M from CHD • Accounts for ~ 12% of congenital cardiac disease in infancy • ~ 75% discharged from hospital w/o diagnosis • ~ 65% - normal newborn screen examination • 6% died before diagnosis • 96% symptoms by 3 wks of life 7 Symptoms Timeline of Clinical Diagnosis Week #1 HLHS Coarctation of aorta TAPVR - obstucted Week #2-6 Transposition of Great Arteries Total Anomalous Venous Return Truncus arteriosus 8 Tetralogy of Fallot Tetralogy of Fallot Prevalence: - 10% of CHD Most common cyanotic heart defect beyond infancy 10 Tetralogy of Fallot +/- Cyanosis Small to Nl cardiac silhouette 11 pulmonary vasculature Tetralogy of Fallot “Tet spell” • Hyperpnea • Worsening cyanosis • Disappearance of murmur • RBBB pattern on ECG 12 Tetralogy of Fallot “Tet spell” • Treatment objectives: Reverse the right-to-left shunt systemic vascular resistance (SVR) Correct potential acidosis with NaHCO3 & volume Consider peripheral vasoconstriction (phenylephrine – 0.02 mg/kg IV) Ketamine – increase SVR and sedates 2 mg/kg over 1 min Morphine sulphate Oxygen 13 Tetralogy of Fallot Surgical Options 14 Blalock-Taussig shunt Trans-annular patch Delayed repair VSD closure Tetralogy of Fallot Post-operative Concerns • Post-pericardiotomy syndrome ~ 4 weeks post-op (25-30% of open heart pts) Fever, elevated ESR and CRP Increased work of breathing (? pericardial effusion) Cardiomegaly, pleural effusions ECG – persistent ST segment elevation with flat or inverted T waves in limb & left lateral limb leads Pericardiocentesis – performed when tamponade physiology present 15 Tetralogy of Fallot Post-operative Concerns • Endocarditis Dx after >2 BCx or echo evidence • Residual VSD • Arrhythmias AV block, ventricular arrhythmias • Remember: Any incision in the ventricle produces a RBBB pattern (rSR’ in V1; wide complex QRS) 16 Tetralogy of Fallot Post-operative Concerns Arrhythmias • TOF - 40% increased incidence of lethal arrhythmias • Syncopal eventslethal ventricular arrhythmias ?? 17 Hypoplastic Left Heart Syndrome HLHS 19 HLHS Uncommon form of cyanotic heart disease Most common cause of death in the first month of life Critically ill infant within the first 7 days with low O2 saturations 20 HLHS Clinically: • Progressive cyanosis and hypoxemia • Hx of poor feeding, tachypnea and poor weight gain • Cardiovascular shock • Severe acidosis • Congestive heart failure 21 Consequences and Complications Polycythemia (erythrocytosis) Clubbing (>6 mos of age) Hypoxic spells CNS • Cyanotic heart disease accounts for 5-10% of brain abscesses • Cerebral venous thrombosis - <2 yrs, cyanotic and microcytic anemia Dyscrasias 22 HLHS Pre-operative Resuscitation Medical management: • Intubation • Ventilate and oxygen • Intravenous access Central/ umbilical/ intra-osseos • Glucose • Na HCO3 • PGE1 (get that PDA open!!) PGE1 0.05 mcg/kg/min • Volume – NS/ 5% Albumin/ PRBC’s • NIRS probe 23 HLHS Norwood/ Blalock-Taussig Shunt Post-operative changes • • • • • • 24 Uncontrolled PBF Re-constructed aortic outflow tract Fluid balance sensitive Widened pulse pressures Tenuous coronary circulation Single ventricle for all circulation HLHS Norwood/ Sano shunt Post-operative changes • Direct PA communication with RV • Uncontrolled PBF • Neo-aortic reconstruction • Higher diastolic pressures • Better coronary perfusion 25 HLHS Post-Operative Resuscitation Limit oxygen (remember: relative uncontrolled PBF) Hemoglobin Auscultate for murmur: • Continuous murmur at RUSB (? BT shunt) • Systolic murmur at RLSB/ LUSB (Sano shunt) Fluid balance: • Palpate liver • +/- rales and CXR to evaluate for CHF • Reverse dehydration Reverse acidosis 26 Coarctation of Aorta Coarctation of Aorta Common cause of left sided heart failure 95% located in juxtaductal region Associated with other congenital anomalies May be short segments or long segments 28 Coarctation of Aorta Associations: • HLHS • Aortic stenosis • TOF • Truncus arteriosus • VSD • DORV • Turner’s syndrome 29 Coarctation of Aorta Clinical • Poor feeding, dyspnea & poor weight gain • Upper arm vs lower extremity BP discrepancy >10-20 mmHg systolic upper vs. lower 20-30% develop CHF by 2-3 months • Hx of lower extremity weakness or pain after exercise • 50% will have no murmur 30 Coarctation of Aorta Acute clinical presentation: • Cardiovascular shock Somnolent & lethargic Poor po intake/ dehydrated, poor U/O Cold, clammy & diaphoretic Poor pulses +/- organomegaly Bradycardia/ tachycardia 31 Coarctation of Aorta Laboratory Evaluation: • CBC & ABG/VBG • CMP, Magnesium & Phos • Lactate • BNP level • CXR & 12 lead ECG • Blood cultures • NIRS probe 32 Coarctation of Aorta Neonatal Coarctation • rSR’ in the right precordial leads (V1 & V2) • Deep S waves in the lateral leads • RAD 33 Coarctation of Aorta Infant Coarctation • LVH apparent (left lateral leads) • Deep S waves in the right chest • Large R waves in lateral leads 34 Coarctation of Aorta Surgical repairs 35 Coarctation of Aorta Post-operative State Re-coarctation • Occurs most commonly within the first 12 months • Evaluated by 4 extremity BP’s • Physical examination of upper & lower extremity pulses 36 Tachyarrhythmia: Sinus Tach vs. SVT Clinical Signs of Tachyarrhythmia 38 Symptoms from History Neonate: • Sudden onset of irritability& sudden relief • Poor po intake & somnolence • Inconsolable • “Rapid heart beat”– felt by parents 39 Older Child: • Stops activity abruptly • “Palpitations”/ “feels funny” • Sudden relief with vasovagal manuever • Chest pain - rare ECG Findings Sinus Tach Sinus Tach 40 Rhythms SVT Regular rhythm, narrow QRS, HR >200, p buried in T wave Sinus Tach 41 Regular rhythm <200, distinct p waves, nl intervals Sinus Tachycardia vs. SVT 42 SVT – Hemodynamically Stable 43 SVT – Hemodynamically Unstable ** Cardioversion should be performed in a location which can provide for continuous monitoring and potential complications of sedation. 44 Medications for SVT 45 Laboratory Evaluation Electrolytes • Calcium, Magnesium & Phosphorus CBC with diff CXR & 12 lead EKG • looking for pre-excitation – WPW 46 Shunt Dependent vs. Non-dependent What’s the big deal !!! The Difference Shunt Dependent • The only source of PBF = SHUNT Non-Dependent • Two sources of PBF = Shunt + some antegrade flow through diminuitive PV 48 Shunt Dependent Oxygen therapy • Limit O2 therapy for cyanosis • Maintain sats 75-85% • Sats can drop significantly and quickly • If sats >85%: PVR PBF Pulmonary edema and circulatory shock • Use blended O2 with range of up to FiO2 0.4 49 Non-Dependent Oxygen therapy • Two sources of PBF: One with fixed obstruction and the other is uncontrolled • If BT shunt present: Limit O2 O2 saturations should not drop as far nor as quickly 50 Summary CHD &/or arrhythmias should be suspected neonates with cardiovascular shock Evaluation should include: • CBC, cultures, electrolytes, lactate levels, Blood gases • CXR, 12 Lead EKG H&P provide 90% of diagnoses 51 Medical Management Airway, Breathing, Circulation What disease and what was the repair? Prostaglandins • 0.03 to 0.1 mcg/kg/min • Side effects: Hyperpyrexia Apnea Flushing 52 Miscellaneous What information do we require? • 4 extremity BP’s, weight %iles • H&P Murmurs Organomegaly Pulses ECG Labs, CXR findings, saturations 53 Sources Internet websites: • www.childrenshospital.org • www.cincinattichildrens.org • www.ucsfhealth.org/childrens/ Pediatric Cardiology for the Practioners. MK Park 4th ed. Congenital Heart Disease - Moss and Adams 54