PowerPoint - American Heart Association
advertisement

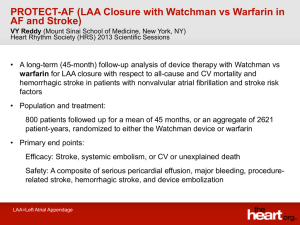
Risks of Intracranial Hemorrhage among Patients with Acute Ischemic Stroke Receiving Warfarin and Treated with Intravenous Tissue Plasminogen Activator Ying Xian, MD, PhD; Li Liang, PhD; Eric E. Smith, MD, MPH; Lee H. Schwamm, MD; Mathew J. Reeves, PhD; DaiWai M. Olson, PhD, RN; Adrian F. Hernandez, MD, MHS; Gregg C. Fonarow, MD; Eric D. Peterson, MD, MPH Presenter Disclosure Information Y Xian, L Liang, MJ Reeves: None EE Smith: Unpaid volunteer for AHA GWTG, Advisory Board to Genentech (2010, <$10,000). LH Schwamm: Dr Schwamm serves as chair of the American Heart Association (AHA) Get With The Guidelines (GWTG) Steering Committee, is a consultant to the Massachusetts Department of Public Health, and provided expert medical opinions in malpractice lawsuits regarding stroke treatment and prevention. DM Olson: Dr Olson reports in the past 2 years receiving no research support, consulting fees, or speaking fees from pharmaceutical companies. He serves as a member of the Duke Clinical Research Institute, which serves as the AHA GWTG data coordinating center. AF Hernandez: Dr Hernandez receives research grant from Johnson & Johnson, Amylin, Proventys and serves as a consultant to Corthera. GC Fonarow: Dr Fonarow receives research support from the National Institutes of Health and previously had served as a consultant to Pfizer, Merck, Schering Plough, Bristol Myers Squibb, and Sanofi-Aventis; previously received speaker honoraria from Pfizer, Merck, Schering Plough, Bristol Myers Squibb, and Sanofi-Aventis, and is an employee of the University of California, which holds a patent on retriever devices for stroke. ED Peterson: Dr Peterson receives research grant from Johnson & Johnson, Eli Lilly and serves as a consultant to Boehringer Ingelheim, Johnson & Johnson, Medscape, Merck, Novartis, Ortho-McNeilJanssen, Pfizer, Westat, Cardiovascular Research Foundation, WebMD, and United Healthcare. DISCLOSURE INFORMATION: Background • Intravenous tissue plasminogen activator (IV tPA) – The most effective medical treatment to improve outcomes for acute ischemic stroke • Symptomatic intracranial hemorrhage (sICH) – A potential life-threatening complication – Incidence: 2.4-8.8% in clinical trials Adams et al, 2007; del Zoppo et al, 2009 Safety of IV tPA in Patients on Warfarin • High prevalence of warfarin use with subtherapeutic INR among ischemic stroke patients • The AHA/ASA stroke guidelines – Patients not taking an oral anticoagulant – If anticoagulant being taken, INR≤1.7 • Lack of safety data of IV tPA in warfarin patients – Excluded from major tPA trials – Few observational studies u Small sample: <250 patients in total u Inconsistent results: odds ratio from 0.29 to 14.7 Adams et al, 2007; Prabhakaran et al, 2010, Meretoja et al, 2010; Kim et al, 2010; Seet et al, 2011; Vergouwen et al, 2011 Objectives • Aim 1: Determine whether warfarin-treated patients were at an increased risk of sICH following IV tPA for acute ischemic stroke. • Aim 2: Examine the association between INR and sICH in warfarin-treated patients. • Aim 3: Estimate the percentage of warfarin-treated patients in current clinical practice who were otherwise eligible to receive tPA treatment, but did not get treated Methods • Study population – Get With The Guidelines-Stroke (GWTG) registry between April 2009-June 2011 u 1/4 of U.S. hospitals u >30% all ischemic stroke cases in the U.S. – 23,437 ischemic stroke patients treated with IV tPA (INR≤1.7) – 1,803 (7.7%) on warfarin • Variables of interest – Warfarin treatment: patient taking warfarin within 7 days of the index stroke admission – Baseline INR: first measurement after presentation to the hospital Outcome Measures • Primary: symptomatic intracranial hemorrhage – Documented ICH by CT or MRI within 36 hours and the treating physician’s notes indicating clinical deterioration, due to hemorrhage • Secondary endpoints – Life-threatening or serious systemic hemorrhage within 36 hours – Any tPA complications within 36 hours – In-hospital mortality Statistical Analysis • Multivariable logistic regression model accounting for within-hospital clustering with GEE approach – Bleeding model: age, gender, race, baseline National Institutes of Health Stroke Scale (NIHSS), systolic blood pressure, and blood glucose – Mortality model: age, gender, arrival mode, medical history of atrial fibrillation, coronary artery disease, prior stroke or transient ischemic attack (TIA), diabetes mellitus, dyslipidemia, and NIHSS – Multiple imputation for 9.9% NIHSS missing data Menon et al, 2012; Smith et al, 2010 Baseline Characteristics Warfarin (N=1,802) No Warfarin (N=21,635) p value 77 (68-84) 71 (59-82) <.001 Female,% 54.2 50.5 .003 Hx of atrial fibrillation,% 69.2 19.0 <.001 Hx of stroke/TIA,% 36.2 26.1 <.001 Hx of CAD/prior MI,% 37.1 27.8 <.001 Hx of heart failure,% 18.0 8.9 <.001 NIHSS, median (IQR) 14 (8-20) 11 (6-17) <.001 1.20 (1.07-1.40) 1.00 (1.00-1.10) <.001 148 (120-174) 145 (115-175) 0.28 53.6 54.9 0.20 Age, median (IQR) INR, median (IQR) Time from symptom onset to IV tPA, median (IQR) Teaching hospital,% Aim 1. Warfarin and Outcomes Endpoints Warfarin (N=1,802) No Warfarin (N=21,635) Adjusted OR (95% CI) p value sICH,% 5.7 4.6 1.01 (0.82-1.25) 0.94 Life-threatening or serious systemic hemorrhage,% 0.9 0.9 0.78 (0.49-1.24) 0.29 Any t-PA complications,% 10.6 8.4 1.09 (0.93-1.29) 0.30 In-hospital mortality,%* 11.4 7.9 0.91 (0.79-1.13) 0.50 * Transfer-out excluded. N=1,772 for warfarin and 21,304 for no warfarin patients Aim 1. Warfarin and sICH, Sensitivity Analysis Main analysis Age<75 years Age 75 years Male Female NIHSS 14 NIHSS>14 Adjustment for antiplatelet Subgroup analysis INR 1.5-1.7 0.0 1.01 (0.82-1.25) 1.12 (0.77-1.62) 0.96 (0.74-1.25) 1.17 (0.87-1.59) 0.89 (0.66-1.19) 1.20 (0.86-1.69) 0.94 (0.70-1.26) 1.04 (0.84-1.29) 1.32 (0.85-2.04) 0.5 1.0 1.5 2.0 Adjusted OR and 95% CI 2.5 Aim 2. INR and sICH in Warfarin Patients (N=1,802) Adjusted OR=1.10, 95% CI (1.00-1.20) for each 0.1 unit increase in INR, p=0.06 Aim 3. Eligible Warfarin Patients Not Receiving IV tPA • 443,916 acute ischemic stroke patients in the GWTG-Stroke Registry Apr 2009-Jun 2011 • 25,762 taking warfarin with INR≤1.7 • 2,489 arrived within 2 hrs w/o contraindication (potentially eligible for 0-3 hr window) • 1,065 arrived between 2-3.5 hrs w/o contraindication (3-4.5 hr window) • 0-3 hr window: 32.1% (799) failed to receive IV tPA • 3-4.5 hr window: 87.3% (930) failed to receive IV tPA • Collectively, 48.6% (1,729/3,554) patients on warfarin who were otherwise eligible were not treated with IV tPA Limitations • Retrospective observational analysis • Potential treatment selection • Lack of long-term outcomes • Generalizability Conclusions • Use of IV tPA among warfarin-treated stroke patients (INR≤1.7) is not associated with increased risks of sICH • While the risk of sICH increases marginally with higher INR, these findings provide empirical support of current AHA/ASA guidelines • Substantial undertreatment among eligible warfarin patients Acknowledgement • • • • Mentor: Eric Peterson Coauthors: Li Liang, Eric Smith, Lee Schwamm, Mathew Reeves, DaiWai Olson, Adrian Hernandez, Gregg Fonarow American Heart Association Pharmaceutical Roundtable and David and Stevie Spina The Get With The Guidelines®–Stroke (GWTG-Stroke) program is provided by the American Heart Association/American Stroke Association. The GWTG-Stroke program is currently supported in part by a charitable contribution from Janssen Pharmaceutical Companies of Johnson & Johnson. GWTG-Stroke has been funded in the past through support from Boeringher-Ingelheim, Merck, Bristol-Myers Squib/Sanofi Pharmaceutical Partnership and the AHA Pharmaceutical Roundtable. 16