cavernoma - Pilgrims Hospital
advertisement

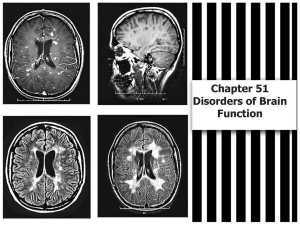
Vascular lesions of the CNS, also known as cerebral cavernous malformations or angiographically-occult arterio-venous malformations Represent a surgically correctable cause of epilepsy in the paediatric population • KM. 9 year old boy • New onset complex partial seizures with right frontal discharges • Seizure activity well-controlled on sodium valproate, levetiracetam, and carbamazepine • Imaging suggested cavernoma Craniotomy & Excision Mesh of thick walled vessels Peri-lesional Haemosiderin Lumen Possible rupture point • MS. 9 year old male • New onset complex partial seizures with right frontal discharges • Seizure activity well-controlled on sodium valproate, levetiracetam, and carbamazepine • Imaging suggested cavernoma • Follow – Up – Seizure frequency ↓ – No deficit • MK. 10 year old girl • 8 month hx of simple & complex partial seizures secondary to right tempero-parietal lesion • Failed multiple single & combination anti-convulsants failed – Side – effects – Fatigue & Poor school performance • Imaging Stealth-guided parietal craniotomy en-bloc resection of lesion + rim of haemosiderin-stained tissue TWV T Hyalinised Thick Walled Vessels [TWV] – Partly thrombosed [T] • MK. 10 year old female • 8 month hx of simple & complex partial seizures secondary to right tempero-parietal lesion • Failed multiple single & combination anti-convulsants failed – Side – effects – Fatigue & Poor school performance • Uneventful post-operative recovery. • Seizure free in immediate post-operative period. • SC. 20 year old woman • 18 yrs → two episodes of new onset seizures • Imaging demonstrated left frontal 2cm x 2 cm lesion, ?? arterio-venous malformation • Carbamazepine initiated. • Cerebral angiography normal Stealth-guided left frontal craniotomy and excision of lesion Lumen Hemosiderin VWR Vessel Wall Remnants [VWR] Elastic Vessel Wall Remnants Siderocalcinosis – perilesional Vascular Malformation remnants – Angio Negative – probable Cavernoma • SC. 20 year old woman • 18 yrs → two episodes of new onset seizures • Imaging demonstrated left frontal 2cm x 2 cm lesion, ?? arterio-venous malformation • Carbamazepine initiated. • Cerebral angiography normal • Uncomplicated recovery and discharged home on post-operative day 4 • Cavernomas may be multiple, ranging from 1-12 • Size range from 0.1cm - 9cm • Risk of haemorrhage estimated to be 2.5% annually [cumulative]. • Risk of new onset seizures is 1.51% annually [cumulative] Most are sporadic. Risk factors include: • previous radiotherapy to brain • more than one first degree relative with cavernoma. • 70% of patients with familial cavernomas carry a frameshift mutation for either KRIT1 / CCM1, MGC4607 / CCM2, or PDCD10 / CCM3, mapping, respectively to chromosomes 7q, 7p, and 3q. • • • • 0.5% of the population ~ 25% diagnosed before age 17 ~ 63 - 81% supratentorial Female preponderance; reason uncertain May present with symptoms secondary to haemorrhage: • new onset seizures • Hydrocephalus [superficial haemosiderosis] • neurological deficit also “Incidentaloma !!!” MRI appearance: • “mulberry” nodules with mixed signal intensity • peripheral haemosiderin rim is seen as an area of decreased signal intensity on T2-weighting and as an area of mixed signal intensity on T1-weighting • no visible feeding vessels, surrounding oedema, or mass effect. Angiographically occult • Dilated sinuses [DS] • Thin vessel walls [TWV] usually lack smooth muscle, elastin, and intervening parenchyma • Electron-microscopy endothelial cells → poorly developed tight junctions, allowing for microhaemorrhages → characteristic haemosiderin staining. • Haemosiderin rim surrounded by reactive gliosis. • Thrombosis [T] may be present DS T TWV 1. Reduces need for long-term anticonvulsants 2. Attainment of intellectual and learning objectives 3. Avoid “labelling” of child as “epileptic” 4. ↓ long-term risk of haemorrhage • Stealth-guided Craniotomies • Excision not only of the cavernoma itself (lesionectomy), but also excision of haemosiderin ring, surrounding gliosis. • In certain cases, may proceed to hippocampectomy. (Varies centre to centre) Seizure control appears to be better in patients who had excision of haemosiderin ring. However, a clear correlation between extent of resection and seizure control has yet to be established. Post-operative seizure control is dependent on: two factors: 1. Length of time the patient was symptomatic pre-operatively. [The shorter the duration of pre-operative seizures, the more likely it is the patient will be seizure-free post-operatively]. 2. ?? Extent of the surgical procedure • Prognosis following surgical excision is usually good • Overall morbidity in most centres is around 4%. • With complete excision of the lesion, the risk of haemorrhage is non-existent. • Cavernomas represent an uncommon but treatable cause of epilepsy and cerebral haemorrhage in the paediatric population. • Symptomatic children diagnosed and treated early will have a better postoperative result References 1. 2. 3. 4. 5. 6. 7. 8. Mottolese C, Hermier M, Stan H, Jouvet A, Saint-Pierre G, Froment JC, Bret P, Lapras C. Central nervous system cavernomas in the pediatric age group. Neurosurg Rev. 2001 Jul;24(2-3):55-71 Labauge P, Brunereau L, Lévy C, Laberge S, Houtteville JP. The natural history of familial cerebral cavernomas: a retrospective MRI study of 40 patients. Neuroradiology. 2000 May;42(5):327-32. Raychaudhuri R, Batjer HH, Awad IA. Intracranial cavernous angioma: a practical review of clinical and biological aspects. Surg Neurol. 2005 Apr;63(4):319-28. Bertalanffy H, Benes L, Miyazawa T, Alberti O, Siegel AM, Sure U. Cerebral cavernomas in the adult. Review of the literature and analysis of 72 surgically treated patients. Neurosurg Rev. 2002 Mar;25(1-2):155. Pinker K, Stavrou I, Knosp E, Trattnig S. Are cerebral cavernomas truly nonenhancing lesions and thereby distinguishable from arteriovenous malformations? MRI findings and histopathological correlation. Magn Reson Imaging. 2006 Jun;24(5):631-7. Chooi WK, Connolly DJ, Coley SC, Griffiths PD. Assessment of blood supply to intracranial pathologies in children using MR digital subtraction angiography. Pediatr Radiol. 2006 Oct;36(10):1057-62. . Pozzati E, Acciarri N, Tognetti F, Marliani F, Giangaspero F. Growth, subsequent bleeding, and de novo appearance of cerebral cavernous angiomas. Neurosurgery. 1996 Apr;38(4):662-70. Sürücü O, Sure U, Gaetzner S, Stahl S, Benes L, Bertalanffy H, Felbor U. Clinical impact of CCM mutation detection in familial cavernous angioma. Childs Nerv Syst. 2006 Nov;22(11):1461-4. T TWV Hyalinised Thick Walled Vessels [TWV] – Partly thrombosed [T] T TWV Hyalinised Thick Walled Vessels [TWV] – Partly thrombosed [T]