Lehigh Valley Health Network - Focus on Respiratory Care & Sleep
advertisement

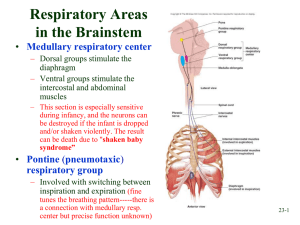
Humidified High Flow Oxygen Therapy Clinical Application Ken Miller, MEd-RRT-NPS Educational/Research Coordinator Respiratory Care LVHN Conflict of Interest I have no real or perceived conflict of interest that relates to this presentation. Any use of brand names is not in any way meant to be an endorsement of a specific product, but to merely illustrate a point of emphasis. Objectives Learning objectives for this presentation: ■ Describe the technological elements of High Flow Oxygen Delivery System. ■ Define the clinical end-points when utilizing High Flow Oxygen Delivery System. ■ Review outcome data and case scenarios with High Flow Oxygen utilization. What is High Flow Oxygen (HFO2) ■ An oxygen delivery system which blends oxygen/air from 35%-100% – Can be administered via wide bore nasal cannula or trach adapter up to 60 L/min. – Provides humidity enriched oxygen therapy for patients in mild to moderate respiratory distress. – HF02 does not augment tidal volume and thus does not facilitate CO2 removal. – It is not a substitute for NIPPV in an acute crisis. – However, it may provide a bridge from NIPPV to conventional oxygen delivery devices and also may give some patients NIPPV free hours. High Flows Oxygen Benefits – There are five key benefits: – Delivers a high FIO2 accurately – Meets the patient’s ventilatory demands – Provides patient comfort – Provides a modest amount of positive airway pressure – Optimizes mucociliary clearance How is High Flow Oxygen Delivered? ■ A combination of: – Molecular high humidification delivery system – An air/oxygen blender – Flowmeter – Via nasal cannula or trach tube adaptor High flow cannula The prongs are wide bore dispersing the flow as it enters the nares and reduces the jetting effect associated with standard nasal cannula Trach adapter Vent Tie-II Utilized for securing Max Venturi Allows for independent control of oxygen and flow Oxygen analyzer FIO2 control Flow rate control 850 Humidifier provides molecular humidification Set a non-invasive mode via cannula Warm Unit for a Minimal of 5’!!! Complete High Flow Oxygen System set up Other High Flow Systems Were Does the Clinician Intervene with HFO2 in the Care Cycle? Invasive ventilation HF02 Non-invasive ventilation Face mask oxygen Humidity therapy HF02 Nasal cannula Advantages of HFO2 PATIENT CLINICIAN Comfortable oxygen delivery, reducing the likelihood of treatment failure Less attendance time assisting uncomfortable patients Can continue to eat, drink, talk and sleep A broad range of flows and oxygen concentrations can be delivered, providing both versatility and continuity of care as patients wean or their condition becomes more acute No need to change between multiple oxygen delivery devices and interfaces Increased confidence in the actual fraction of inspired oxygen (FiO2) being delivered to the patient May displace the need for noninvasive or invasive ventilation through better patient tolerance Easier oral care, maintaining the moisture in the oral mucosa Better secretion clearance, reducing the May be used to wean patients off risk of respiratory noninvasive or invasive ventilation infection High Flows of Oxygen Delivered Through Nasal Cannula ■ The combination of nasal cannula and optimal humidity enables comfortable delivery of high flows Patient comfort Optimized patient outcomes Patient compliance Octoberfest Party Last Year!!! hoping next year’s Octoberfest::) I Why Improvement in Oxygenation? ■ Guaranteed FI02 delivered ■ Ventilatory demands met ■ “Back pressure CPAP” -Every ten liters of flow approximately 1 cm of CPAP is generated! -Maximum of 5-6cm CPAP can be achieved. Meeting patient’s inspiratory flow demand No ambient entrainment Face-mask oxygen delivery vs High Flow Oxygen Approximately 1 cm/h20 of “back pressure CPAP” per every ten liters of flow HFO can not help here!!! Adequate hydration Inadequate humification : Where to Start High Flow Oxygen 70% FI02 40 lpm SpO2 Monitoring ■ ■ A SpO2 monitor is to be utilized for ALL HFO2 patients and low SpO2 alarm must be set 2% below the physician ordered desired Sp02. The high respiratory rate alarm must also be set per physician order on the appropriate bedside monitor. Weaning of HFO2 ■ ■ ■ Titrate to 40% oxygen Reduce Flow to 20-30LPM Transition to nasal cannula Does this really work??? Outcomes ■ ■ Sixty patients were placed on HFNC from July 1, 2009 to Dec 31, 2009 in MSICU. In the HFNC that did not required therapy escalation had a 11.5 duration in MSICU compared to 19.5 who did. 20 18 16 14 12 10 8 6 4 2 0 HFNC BPAP/ Vent Clinical Indications 45 40 35 30 25 20 15 10 5 0 Oxygenation Ventilatory demands Humidification st O Optiflow Diagnosis eu m on ia M ISC DX Re sp M is c Pn p Bu rn Tr au m a/ Po PD CH F CO Number of Patients 2009-2011 Patient Diagnosis 80 60 40 20 0 New Data 2011-12 120 100 80 60 40 20 0 Total Oxygen Trach Oxygen BIPAP/Vent ICU LOS 2011-2012 18 16 14 12 Oxygen BIPAP Vent 10 8 6 4 2 0 ICU stay Hypothesis ■ HFO may reduce escalation of therapy in specific patient populations that exhibit certain clinical and demographic characteristics Relevance to Practice ■ ■ ■ ■ Aid clinical decision making as to whether or not HFO is the best option for a specific patient Initiate HFO on patients that display characteristics deemed successful Not consider HFO for patients that display characteristics deemed unsuccessful Effective and efficient use of respiratory technology Study Design ■ ■ ■ ■ ■ ■ Retrospective observational study Analyzed data on patients at LVHN who were placed on HFO from May 21, 2011 to May 21, 2012 Sample size: 137 patients Patients less than 18-years-old were excluded Patients on HFO were identified from a daily report received by respiratory therapy Electronic medical record was used to gather demographic and clinical information regarding these patients Methods ■ Patients were separated into two groups: patients who were successful on HFO and patients who were not ■ Success was defined as de-escalation in care, meaning the patient maintained clinical end-points on HFO or conventional oxygen delivery systems ■ Failure was defined as escalation in care, meaning that in order to maintain desired clinical end-points either NIPPV or mechanical ventilation had to be instituted ■ If a patient was on HFO for more than 72 hours they were counted as a failure because HFO is not indicated to be a longterm therapy1 Results ■ ■ ■ ■ All variables which were found to be statistically different (p<0.05) between the two groups were included in the logistic regression model. Patients who had a previously existing co-morbidity of pulmonary disease were 5.81(p=0.023) times more likely to fail on HFO compared to patients who did not have a previously existing co-morbidity of pulmonary disease. For every one day increase in ICU length-of-stay the odds of failing on HFO increased by 1.14 (p=0.001). Compared to those who were on HFO for 0 to 4 hours, those who were on HFO for greater than 16 hours were 13.11 (p=0.001) times more likely to be a success. Interpretation/Conclusion ■ Patients who stay in the ICU for a longer period of time may be more likely to fail on HFO because these individuals tend to be sicker. ■ Those who are going to fail on HFO are more likely to do so in the first sixteen hours, therefore, these hours are crucial for the patient. ■ Patients who have a previously existing comorbidity of pulmonary disease are more likely to fail on HFO. ■ Patients who succeed on HFO spend an average of 7.63 days in the ICU compared to 14.83 days for patients who fail. High Flow Oxygen Results 2011-2012 600 500 400 300 200 100 0 Total NC Trach High Flow Oxygen Results Indications 2011-2012 Oxygenation NIPPV Free Vent Liberation WOB Secretions Palliative 294 42 57 49 77 30 HFO Results Outcomes 2012 350 300 250 200 150 100 50 0 Oxygen NIPPV Mech Vent Comfort Literature Outcomes ■ High-flow oxygen therapy in acute respiratory failure. Roca O, Riera J, Torres F, Masclans JR. Servei de Medicina Intensiva (Area General), Hospital Universitari Vall d'Hebron, Passeig Vall d'Hebron 119-129, 08035 Barcelona, Spain. oroca@ir.vhebron.net ■ CONCLUSIONS: HFNC was better tolerated and more comfortable than face mask. HFNC was associated with better oxygenation and lower respiratory rate. HFNC could have an important role in the treatment of patients with acute respiratory failure. ■ High-Flow Oxygen Administration by Nasal Cannula for Adult and Perinatal Patients Jeffrey J Ward MEd RRT FAARC: ■ The HFNC can effectively be used to treat patients with moderate levels of hypoxemic respiratory failure. HFNC could be considered as an initial appliance in certain settings (eg, ED), as flow could be titrated based on response over a full range without having to change to other devices. Case Scenarios ■ ■ ■ ■ ■ ■ ■ Post liberation from long-duration Mechanical Ventilation Inability to administer mask either for high flow Oxygen Delivery or NIPPV secondary to facial surgical graft Bridge therapy from NIPPV to conventional Oxygen Administration In lieu of CPAP Intervention Nitric Oxide/Heliox Administration Post extubation Pulmonary Edema Patient comfort—Palliative Care Nurse’s reaction when I bring new technology into her room!! Liberation Following Prolong Ventilatory Support ■ A twenty-seven year old female was admitted to our ICU for Pneumonia and Sepsis. She developed full-blown ARDS and required full ventilatory support for fifty-two days. ■ She received a tracheostomy on day thirty-two and required prolonged periods of FIO2 >60% to maintain a Sp02>88%. Several bronchoscopies were performed to address mucus plugging and maintain a patent airway. She was slowly transition to partial ventilatory support and then attempts were made to conduct spontaneous breathing trials (SBT) via conventional high flow oxygen system utilizing a trach mask/ttube. During the breathing trials the patient’s respiratory rate and heart rate increased above clinical end-points and a paradoxical breathing pattern with associated wheezing was noted. Secretion removal was also problematic, requiring frequent suctioning. Periods of desaturation were noted requiring titration of oxygen delivery >60%. After four days of failed SBTs the patient was placed HFO2 via trach adapter. After institution of this oxygen and humidification delivery system, periods of desaturations were absent and work of breathing was reduced. Stable hemodynamics and airway patency were maintained. The patient remained liberated from mechanical ventilation and was transferred to a long-term care facility. Inability to Administer Mask Either for High Flow Oxygen Delivery or BIPAP Secondary to Facial Surgical Graft ■ A thirty-nine year old male received a right superficial parotidectomy modified neck dissection for dermatofibrosarcoma. The operative procedure lasted fourteen hours and the patient was chemically paralyzed for medical stability and required mechanical ventilation for five days. ■ During the ventilatory duration, the patient developed pneumonia which was resolved with antibiotic administration. The patient was extubated on day six but required reintubation within six hours, secondary to excessive work of breathing and hypoxemia. High flow oxygen administration or non-invasive positive pressure ventilation were not options secondary to the location and fragile state of the facial skin graft. Mechanical ventilation was continued for an additional five days. The patient was then extubated and placed on HFNC, set at fifty percent oxygen and with a flow of thirty liters per minute. SpO2 was maintained>93% and work of breathing was minimal, secretion removal was adequate. The patient was transferred to medical-surgical unit within twentyfour hours. Bridge Therapy from NIPPV to Conventional Oxygen Administration ■ An eighty-two year old female was placed on NIPPV for Respiratory Failure. Attempts to wean off NIPPV failed secondary to desaturation and increased WOB. ■ HFNC was placed on the patient at 60% and 40LPM, SPO2 was maintained and the patient remained NIPPV until discharge to a longterm skilled care facility. Post Extubation Pulmonary Edema ■ ■ A thirty-two year old male was admitted for bacterial pneumonia who required mechanical ventilation for seven days. Decision was made to attempt ventilatory liberation, weaning parameters were adequate however cardiac function was marginal. Decision was made to extubate, which was performed. Within two minutes post extubation the patient develop acute pulmonary edema and had to be re-intubated and ventilated. Post forty eight hours post extubation failure the decision again was made to attempt ventilatory liberation. At this point to minimize the lost of positive pressure post extubation, HFNC was placed in the patient’s nares set at 50 lpm and 50%, extubated was performed and the clinical course remained stable. HFNC Via Heliox ■ ■ ■ Seventy-one year old patient admitted with a laryngeal tumor was placed on NIPPV along with Heliox. Patient vomited multiple times and mask compliance was marginal associated with desaturation and increased work of breathing. Patient was placed on HFNC via Heliox gas exchange stabilized and patient compliance was adhere to. Patient Comfort ■ ■ ■ A fifty-five year old female was admitted for aortic value insufficiency a with a history if idiopathic pulmonary fibrosis. The patient under went aortic value repair. Post operatively she had multiple bouts of respiratory failure and required prolong mechanical ventilation. She was transited to NIPPV post ventilatory liberation and required its utilization for prolonged periods of time. To enhance the patient’s ability to communicate to her family and to have longer durations of BIPAP free-time to enjoy her meals HFNC was instituted. Post HFNC , NIPPV utilization was been reduced to hours of sleep only. High-flow Oxygen System Clinical Indications Met? 1 Warm Unit for 5’ Set FIO2 to Maintain Sp02>93% Set LPM 40LPM Increase FI02 or Liter flow Sp02>93% Yes Sp02>93% 3 Increase Flow to 50-60LPM No Is Patient’s Inspiratory Flow Met? Yes Maintain/wean Current Settings No Maintain Current Settings Yes 4 No Clinical Status Stable? Maintain Current Settings Yes No No Is Patient’s Inspiratory Flow Met? Yes 2 Re-assess for other clinical interventions No Clinical Status Stable? 6 Maintain/wean Current Settings Yes 5 Place on Conventional Oxygen System 8 7 Transferred From Critical Care FIO2< 60% Flow<40Lpm HFO2 ■ ■ ■ ■ ■ ■ Provides wide range of precise FIO2 delivery for many patient populations Enhances muco-kinesis Provides a pseudo-CPAP Maintains sufficient flow to maintain the patient’s inspiratory flow demands Easy to administer and maintain Patient comfort Unanswered Questions!!! ■ HFO effect on mortality? It’s effect on ICU duration in a randomized controlled study? ■ Can it be used safely during an acute crisis in medical-surgical patient population? ■ Kenneth Miller MEd, RRT-ACCS, RRT-NPS Respiratory Care LVHN 610-402-5772 Kenneth.miller@lvhn.org