OS Odontoideum
advertisement

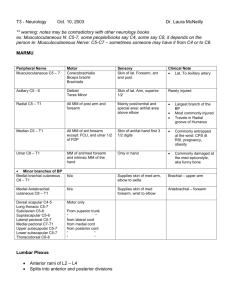
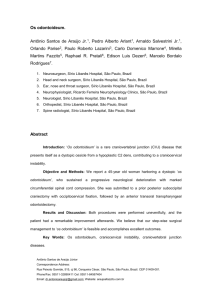
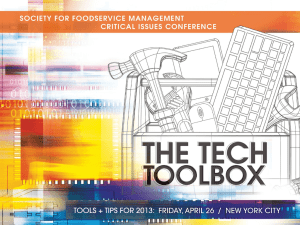
Atul Gupta Neuroradiology Overview Os odontoideum (OO) is an uncommon craniovertebral junction (CVJ) abnormality characterized by a separate ossicle superior to the dens. Location: Orthotopic – In normal position at tip of dens Dystopic – Displaced towards base of occiput where it may fuse w/clivus or anterior ring of C1. Associated w/hypoplastic dens Spinal canal may narrowed in both types Size/shape vary, smooth cortical borders Leads to atlanto-axial instability (both types) Transverse atlantal ligament is ineffective at restraining atlantoaxial motion. B A C Dystopic OO. A. Coronal CT shows OO (arrow) fused with clivus. B. Coronal CT shows incomplete (right) C1. C. Axial view shows clefts involving C1 anteriorly & posteriorly & a dysplastic C2. Dystopic OO. Midsagittal T1 WI shows large OO (arrow) fused with clivus, small anterior arch of C1, & narrowed spinal canal. A B Orthotopic OO. A. Sagittal CT shows large OO (arrow) not fused with clivus but angled slightly anterior. B. Corresponding MR T1WI shows narrowed spinal canal. Causes Trauma Congenital: Increased incidence in: ○ Morquio syndrome ○ Multiple epiphyseal dysplasia ○ Down’s Syndrome There is continuing controversy over its etiology Diagnosis o o Usually incidentally detected or when symptoms occur Open-mouth, anterior-posterior, and flexionextension lateral radiographs o Gap separating the OO and axis proper should be above level of superior articular facets o Hypertrophy of anterior arch of C1 o o o 1 mm cuts sagittal CT reconstruction give more detail into the atlanto-axial junction MRI – can help visualize spinal cord pathology, show space available for cord and provide ant-post canal dimensions Fluoroscopy is recommended to show instability A B Orthotopic OO. Flexion (A) & extension (B) radiographs show widening of atlantodental interval compatible with subluxation & instability. Differential Diagnosis Persistent ossiculum terminale True hypoplasia of odontoid peg Neurocentral synchondrosis Odontoid fracture nonunion Symptoms Predisposes to increased risk of craniovertebral junction trauma Acute neurological dysfunction with an insidious onset and: Torticollis Localized pain Neurovascular compromise signs Cervicomedullary compromise may require neurosurgery in irreducible cranio-cervical stenosis. Treatment Monitor diagnosed patient for: Motor dynamics – look for increase in multidirectional movement at cranio-vertabral junction indicating increased laxity of secondary ligaments Monitor for neurological signs Dorsal arthrodesis Posterior atlantoaxial onlay fusion Posterior atlantoaxial wiring and fusion Posterior occipitocervical wiring and fusion Posterior Magerl screw fixation and fusion Harms technique of C1-2 fusion Anterior resection of the os fragment Posterior transarticular screw fixation