Eosinophilic Esophagitis Endoscopy
advertisement

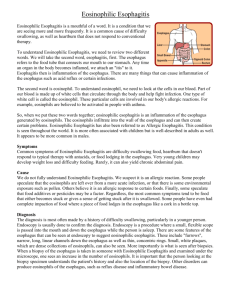
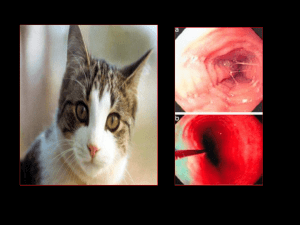
EOSINOPHILIC ESOPHAGITIS EOSINOPHILIC ESOPHAGITIS DISEASE WITH MANY NAMES Congenital esophageal stenosis Feline esophagus Ringed esophagus Corrugated esophagus Small caliber esophagus Stiff or non-compliant esophagus DIAGNOSTIC GUIDELINES OF EOSINOPHILIC ESOPHAGITIS • Clinical symptoms of esophageal dysfunction • More than 15 eosinophil in 1hpf ( x400) • Lack of response to high dose ppi (2mg/kg/d) Or • Normal pH monitoring of distal esophagus EOSINOPHILIC ESOPHAGITIS DEMOGRAPHICS AND PRESENTING SYMPTOMS • • • • • Male gender: 75% Age: mean between 36 to 42 yrs Westernized countries: US, Europe, Australia, Japan May be seen in other first degree relatives Presenting symptoms: Dysphagia: >90% Food impaction: 50% Heartburn: 33% Chest pain/vomiting Most carry a diagnosis of GERD • Extraesophageal symptoms: Asthma: 50% food allergies: 10-30% Potter JW GI Endo 2004, Desai TK GI Endo 2005, Remedios M GI Endo 2005 Differential Diagnosis of Esophageal Eosinophilia • GERD • Eosinophilic esophagitis • Eosinophilic gastroenteritis • Crohn’s disease • Connective tissue disease • Hypereosinophilic syndrome • Infection • Drug hypersensitivity response Symptoms Suggestive of Eosinophilic Esophagitis CHILDREN Feeding aversion/intolerance Vomiting/regurgitation “GERD refractory to ppi “ “GERD refractory to surgical rx” Food or foreign body impaction Epigastric pain Dysphagia Failure to thrive Slow eating ADULT Dysphagia Food impaction “GERD refractory to ppi” Slow eating Heartburn RINGED ESOPHAGUS Endoscopic Features Associated With Eosinophilic Esophagitis • Linear furrowing, vertical lines of the esophageal mucosa • White exudates, white specks, nodule, granularity • Circular rings, transient or fixed, felinization • Linear shearing/ crepe paper mucosa with passage of endoscope or dilator • Stricture: proximal, middle, or distal • Normal EOSINOPHILIC ESOPHAGITIS Histologic Features Associated with Eosinophilic Esophagitis • More than 15 intraepithelial eos/ 1 HPF • Eosinophil microabcess • Superficial layering of eosinophils • Basal zone hyperplasia • Increase papillary height • Increase in lamina propria and papillae fibrosis ESOPHAGEAL EOSINOPHILIA WITH DYSPHAGIA AND NORMAL ENDOSCOPY • 12 patients (10M, 32yrs) with > 20 eos/HPF • 3 pts 1986-88 and 9 pts between 1988-1990 • All had dysphagia with normal endoscopy • 7 had hypersensitivity (3 asthma) and 1periph eosinophila • esophageal manometry- nonspecific EMD in 10 and normal LES in all • Esophagel pH- abnormal in 1 • Treatment- all required frequent dilatations, one resolved with oral steroids Treatment Of Eosinophilic Esophagitis • • • • • • • • • Acid suppression Esophageal dilatation Elimination diets Systemic corticosteroids Topical corticosteroids Antihistamines and cromolyn Montelukast (leukotriene inhibitor, Singulair) Mepolizumab (anti IL-5) Purine analogues (Azathioprine or 6MP) USE OF INHALED STEROIDS IN EOSINOPHILIC ESOPHAGITIS • Fluticasone 4 puffs (220mcg/puff) • Twice daily before breakfast and dinner • Duration: 6 weeks • Insure delivery to esophagus by removing the spacer • Inspire deeply, depress the inhaler, and swallow the aerosol • Rinse mouth with water and avoid food and drink for 1-3 hours ORAL PREDNISONE VS TOPICAL FLUTICASONE IN TREATMENT OF EOSINOPHILIC ESOPHAGITIS • Systemic and topical steroids are effective in achieving histologic and clinical improvement • Prednisone results in greater histologic improvement, without associated clinical advantage over fluticasone • Symptom relapse is common in both group upon therapy discontinuation Clinical Gastroentrol and Hepatol 2008;6:165-173 MONTELUKAST IN EOSINOPHILIC ESOPHAGITIS • Montelukast (Singulair) is leukotriene receptor antagonist which blocks leukotriene D4 receptors, reducing the inflammatory action of eosinophils • 8 patients with EE with montelukast - starting dose 10 mg AM increased to 100 mg - maintenance dose: 20-40 mg/day • 6 of 8 reported complete resolution of dysphagia with median 14 months follow-up • However, esophageal eosinophilia persisted • Side effects: nausea, myalgias Attwood SE et al. Gut 2003 EOSINOPHILIC ESOPHAGITIS ESOPHAGEAL TEARS AND PERFORATION • Esophageal tears or rents in the muscle layer may occur even with passage of endoscope • Frequency is variable -Kaplan 5/8 (63%) -Potter 10/13 (77%) -Younes 1/10 (10%) mean 3 year fu- no further dilatations -Straumann 0/11-mean fu 7 yrs 7 once and 4 repeated dilatations • No evidence of true perforation- but painful in some needing narcotics • Key: start small caliber < 10 mm dilator, gradually advance and stop with blood on bougie Kaplan Clin Gastro Hep 2003, Younes Dig Dis 1999, Strauman Gastro 2003 EXAMPLE CASE A 22 year old man for the evaluation of solid food dysphagia. He has had 2 episodes of food impaction in the last year. He is a slow eater, solid foods stick intermittently in the midchest, but no liquid dysphagia. Rare heartburn but no weight loss. History of mild asthma since childhood and can’t eat some nuts. Omeprazole hasn’t helped Physical exam and complete blood count is unremarkable
![EOSINOPHILIC ESOPHAGITIS [EE]](http://s3.studylib.net/store/data/009399872_1-fb87975e549aa57f606b438a42821700-300x300.png)