Definition:
Primary malignant tumors of lymphoid
tissue, they represent 5% of all malignant
tumors.
Incidence:
Male: Female
HD.
N.H.L.
2:1
1.4 : 1
According to the U.S. National
Institutes of Health, lymphomas
account for about five percent of
all cases of cancer in the United
States, and Hodgkin's lymphoma
in particular accounts for less
than one percent of all cases of
cancer in the United States.
Because the whole system is
part of the body's immune
system, patients with a
weakened immune system, such
as from HIV infection or from
certain drugs or medication, also
have a higher incidence of
lymphoma.
Aetiology of Predisposing factors:
1- Hodgkin’s disease :
a-Infectious aetiology (may be initiated by an infection but
may not be transmitted)
*may be hypersensitive immune response to a virus.
*relation to Ebstein Barr virus as evidenced by:
- +ve antibodies
- Increase incidence in-patient with inf.
Ononucleosis
b-Abnormal immune response
- depression of cellular immunity should be
considered an inherent character of the patient
who ultimatIy develop H.D
2-Non Hodgkin’s lymphoma:
* Neoplasia of the immune system
* Can be considered is a disorder of lymphoid
differentiation.
Possible Aetiologic factors of NHL:
I-Host Factors:a- Primary Immune deficiency
b- Immuno suppressive ttt.
2-Invironmental Factors:a- Ionizing radiations.
b-Drugs: (Hydantion, Anaesthesia)
c- Chemicals: (Petrol. Viny1 Chloride)
d- E.B.V
Age Incidence:-
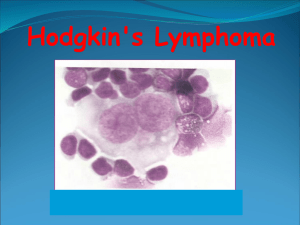
Histopathology:1- H.D.:
Disease of Lymphatic tissue characterized by the
presence of Reed Sternberg cells and variable proliferations
of lymphocytes.
*Rye Classification
Sub Type
Lymphatic predominance (L.P.)
Nodular sclerosis (N.S.)
Mixed Cellularity (MC.)
Lymphocytic Deplition (L.D.)
Average %
10 – 12%
45 - 55%
30 - 35%
8- 10%
L.P., or, N.S. are more favourable than M.C and L.D.
Classifications
of
Non Hodgkin’s Lymphoma
Many classifications according toHistopathology:-
a-Rappaport classification:- depends on:
1-Pattern of growth:-
- Nodular (N.) [ Follicular, Indolent]
- Diffuse (D.) [Aggressive]
2- Cell population:
- Lymphocytic (L.)
- Histiocytic (H.)
- Mixed (L & H.)
Types :
* Favorable histology: N.L.,N. Mixed, DL.W.D(well differentiated)
*Unfavorable histology: N.H. + all D., except DL. W.D
* Histioocytic of several varities:
- majority (large cell L. immunoblastic L.)
- true H is very rare
B-A number of different classification
systems exist for lymphoma.
Kiel:
Karl Lennert of Kiel, Germany, proposed
a new system of classifying lymphomas
based on cellular morphology and their
relationship to cells of the normal
peripheral lymphoid system
REAL:
In the mid 1990s, the Revised
European-American Lymphoma
(REAL) Classification attempted to
apply immunophenotypic and genetic
features in identifying distinct
clinicopathologic NHL entities
C-Working Formulation:
I- Low Grade Malignancy:
- small lymphocytic (C.L.L.)
- Follicular small cleaved.
- Follicular mixed small and large cleaved.
2- Intermediate Grade Malignancy:
- Follicular large cell
- Diffuse small cleaved
- Diffuse mixed small and large cells.
- Diffuse large cells: i- cleaved
ii- non cleaved
3- High Grade Malignancy:
- Immunoblastic Lymphoma.
- Lymphoblastic Lymphoma
- Small non cleaved (Burkitt’s)
*In NHL: The presence of a
nodular pattern (follicular)
remains
an
important
prognostic feature in addition
to the cell type
D-WHO Classification:
The WHO Classification,
published in 2001 and updated
in 2008, is the latest
classification of lymphoma .
This system attempts to group
lymphomas by cell type (i.e.
the normal cell type that most
resembles the tumour) and
defining phenotypic, molecular
or cytogenetic characteristics.
There are three large groups: the
B cell, T cell, and natural killer cell
tumours. Other less common
groups, are also recognized.
Hodgkin's lymphoma, although
considered separately within the
WHO classifications, is now
recognized as being a tumour of,
albeit markedly abnormal,
lymphocytes of mature B cell
lineage
-1-Mature B cell neoplasms:
.
•Chronic lymphocytic leukemia/Small lymphocytic lymphoma
•B-cell prolymphocytic leukemia
•Lymphoplasmacytic lymphoma (such as Waldenström macroglobulinemia)
•Splenic marginal zone lymphoma
•Plasma cell neoplasms:
•Plasma cell myeloma
•Plasmacytoma
•
•Heavy chain diseases
•Extranodal marginal zone B cell lymphoma, also called MALT lymphoma
•Nodal marginal zone B cell lymphoma (NMZL)
•Follicular lymphoma
•Mantle cell lymphoma
•Diffuse large B cell lymphoma
•Mediastinal (thymic) large B cell lymphoma
•
•Primary effusion lymphoma
•Burkitt lymphoma/leukemia
-2-Mature T cell and natural killer (NK)
neoplasms:cell
T cell prolymphocytic leukemia
T cell large granular lymphocytic leukemia
Aggressive NK cell leukemia
Adult T cell leukemia/lymphoma
Extranodal NK/T cell lymphoma, nasal type
Enteropathy-type T cell lymphoma
Hepatosplenic T cell lymphoma
Blastic NK cell lymphoma
Mycosis fungoides / Sezary syndrome
Primary cutaneous CD30-positive T cell
lymphoproliferative disorders
Primary cutaneous anaplastic large cell lymphoma
Lymphomatoid papulosis
Angioimmunoblastic T cell lymphoma
Peripheral T cell lymphoma, unspecified
Anaplastic large cell lymphoma
-3-Hodgkin lymphoma
Classical Hodgkin lymphomas:
*Nodular sclerosis
Mixed cellularity
*Lymphocyte-rich
*Lymphocyte depleted or not
depleted
*Nodular lymphocyte-predominant
Hodgkin lymphoma
-4-Immunodeficiency-associated
lymphoproliferative disorders:
*Associated with a primary immune disorder
*Associated with the Human Immunodeficiency
Virus (HIV)
*Post-transplant
*Associated with methotrexate therapy
General Considerations:
I-H-D.:
* usually have a unicentric origin & usually
starts by involvement L.N. in one or more adjacent areas
esp. in cervical region.
N.H.L. :
* usually multicentric from the start.
* in 1/3 onset occur in extranodal sites.
2- Mode of spread:
H. D.
* in the great majority via lymphatics to
contagious L.N. and other lymphatic structures
N.H.L. :
* more often rapidly spread to distant nodal
and extranodal sites via blood stream
1- Asymptomatic Lymphadenopathy:-
* the majority of patients with H.D. (extranodal
only in 10%) .
* 2/3 of patients with N.H.L. (1/3 extranodal).
Usually in cervical L.N.(cervical onset 65- 80%,
in H.D. ,while in N.H.L. only in 30 - 40%).
a-H.D.:
*Characterized by central
L.N. involvement (cervical,
mediastinal & para-aortic) esp. in N.S. subtype
* Certain groups of L.N are rarely involved in H.D.:
- epitrochlear, popliteal.
- mesentric, hypogastric
- hepatic, hilar.
* 10-20% of early stage H.D. is presented with mediastinal L.N.
but higher incidence with N.S. and is usually associated systemic
symptoms.
N.B L.N in H.D. are firm rubbery (not stoney hard), non-tender
(except if rapid enlargement), equal in size in each group, initially
discrete.
b-N.H.L.:
*More widely disseminated in nodal and
extranodal sites.
*L.N. distribution is often peripheral (axillary,
inguinal, mesentric).
*Mediastinal L.N. in less than 15% and only in
aggressive
lymphoma
esp
Lymphoblastic
lymphoma.
2-Extra Nodal Lesions:
*In N.H.L.: the most commonly involved sites are the
head & neck areas (Waldeyer’s ring, nasal cavities,
sinuses & orbit) followed by G.I.T.
*In H.D.: splenic & hepatic involvement esp. in
presence of :-L.N enlargement above and below the
diaphragm.
-systemic symptoms
- and in M.C and L.D. subtypes.
N.B Hepatic involvement usually in association with
concomitant splenic involvement.
a-G.I.T.:
* diarrhoea , malabsorption syndrom ( G.I.T. infiltration)
* ulceration & bleeding.
* retroperitoneal masses esp. in N.H.L. resulting in I.V.C
obstruction, leading to ascitis and oedema.
Primary GI N.H.L:
- Adults: stomach > intestine.
- Children: intestine > stomach esp. for Burkitt’s
(iliocaecal valve)
-There is association between affection of Waldeyer's ring
& G.I. lymphoma esp. the stomach.
Jaundice in H.D: may be due to:
- intrahepatic cholestasis: involvement of portal tracts.
- extrahepatic cholestasis due to glands in porta hepatis.
- auto immune haemolytic anaemia.
b- Chest:
* involvement of lung parenchyma (nodules,
cavitations).
* usually due to infiltration by contiguity from
adenopathy .
* Pleural and / or pericardial involvement (usually with
massive mediastinal L.N. enlargement.)
* massive mediastinal L.N. enlargement leading to
mediastinal syndrome esp. with :
- N.S. (H.D.)
- Lymphoblastic (N.H.L.)
C-Bone Pain & Tenderness:
* may be oesteolytic or oesteoblastic and may be
pathological fractures.
d- Neurological Manifestation;
* Herpes Zoster.
* Spinal cord compression (H.D.) .
* Peripheral nerve palsies. [Horner's, brachial plexus,
phrenic nerve, vocal cords].
* Cranial nerve palsies.
* Cerebral signs and symptoms
e-Cutaneous Manifestations:* Pruritis
* Skin nodules.
* Herpes zoster
* Alopecia and icthyosis
* Hyperpigmentation.
3- Systemic or constitutional symptoms:
* May occur with L.N. enlargement or may precedes it.
* Common with H.D. (30-40%) than N.H.L. (10%).
* Fever > 38 ,night sweats, wt . loss, pruritis, other systemic
symptoms.
* Alcohol intolerance (H.D.):
- localized acute pain at one or more sites of Hodgkin's
involvement
- anorexia, malaise. fatigue
* Systemic symptoms means unfavorable prognosis.
Diagnostic Evaluation and Staging:
Proper ttt depends on:
- Hisopathologic Type.
- Anatomic extent of
disease (staging)
*Diagnosis:
- The precise unequivocal diagnosis requires
histopathologic confirmation by the examination of
suitable biopsy material.
- Most satisfactory nodes: (lower cervical &
axillary).
- If there is a group of L.N. take the central ones.
- If there is only mediastinal L.N.:(mediastinascopy
or thoracotomy).
Hodgkin’s lymphoma.
Lymph node with CD30-positive Hodgkin
cells and binucleated Reed-Stemberg cells.
Immunophenotyping is an
important diagnostic modality
and is crucial for the classifi
cation of non-Hodgkin’s
lymphoma. Certain markers,
such as the CD-20 receptor,
have become crucial for
treatment as newer biologic
agents have utilized this
receptor therapeutically
.
Classical HL
Characteristic Reed-Sternberg cell
cell
Surface antigens CD15+,CD30+,
CD20+/–, CD45–,
EMA–
EBV
+EBV in 50%
NLPHL
Lymphocytic and
histiocytic cell
“popcorn cells”
CD15–, CD30–,
CD20+, CD45+,
EMA+
EBV–
NLPHL is the most favorable HL
with an indolent course.
Clinical Staging:
I- Detailed history esp. systemic symptoms.
2- Clinical exam. including Waldeyer's ring, areas of
bone tenderness.
3- Adequate surgical biopsy
4- Routine laboratory tests(CBC,ESR. liver function
test, serum uric acid)
5- Plain chest X ray & bilateral lower extremity
lymphangiography.
6- Radiologic examination of GIT & gastroscopy. If +ve
Waldeyer's ring.
Imaging and laboratory work-ups
for non-Hodgkin’s lymphoma
Imaging studies
■ Laboratory tests
– CT scan of chest, abdomen, – Complete blood
and pelvis
count
– FDG-PET scan or PET/CT
– Serum chemistry
– Gallium-67 scan (if PET
– Lactate dehydro
unavailable)
genase (LDH)
– MRI or CT of the brain
– Liver function tests
(if symptomatically indicated) – Renal function tests
– Bone scan
– Erythrocyte sedi-
(if symptomatically indicated) mentation rate (ESR)
Positron emission tomography (PET) using
fluorodeoxyglucose has been found useful for the
staging and follow-up of patients with HL. PET is
sensitive and, in most instances, specific enough
to detect involvement by HL. In untreated
patients, a higher stage is found in at least 20%
of cases using PET imaging as compared with
conventional imaging. PET may also be used in
patients with residual tumor masses to
discriminate
Pathologic staging:
1- Bone marrow biopsy
2- Staging laparotomy, after -ve bone narrow
biopsy in Clinical stage I & II H.D.
3- Lumbar puncture with cytologic exam. Of
C.S.F in all N.H.L with bone marrow
involvement.
4- Cytologic exam. of any effusion
The Ann Arbor staging
:mentioned before.
classification
Bone marrow biopsy (bilateral) is
recommended for all cases of NHL
because of the high probability of bone
marrow involvement for certain types of
NHL in : 70% in small lymphocytic
lymphoma, 50% in follicular lymphoma,
and >10% in diffuse large-cell lymphoma or marginal zone lymphoma.
Cytological examination of cranial spinal
fluid (CSF) is indicated for stage IV
disease with bone marrow, testis, and
parameningeal involvement .
Ann Arbor staging system
Stage I Involvement of single lymph node (I) or extralymphatic site (IE)
Involvement of two or more involved lymph node sites on the
Stage II same side of the diaphragm (II) or localized involvement of one
extra-lymphatic organ or site plus one or more lymph node
regions on the same side of diaphragm (IIE)
Involvement of lymph node regions on both sides of diaphragm
Stage III (III), which can also include involvement of the spleen (IIIS) or
localized extralymphatic site or organ extension (IIIE) or both
(IIISE)
Stage IV Diffuse (multifocal) involvement of one or more extralymphatic
organs or sites
A=No “B” symptoms B=Unexplained fever >38°C, weight loss
>10% in previous 6 months, drenching night sweats X=Bulky
disease
Prognostic Factors:
Histology subtype of lymphoma is the most important
determinant of prognosis of non-Hodg-kin’s lymphoma.
■ NHL of certain origins, such as primary CNS lymphoma and
testicular NHL, have particularly poor outcome after treatment.
■ The presenting stage is an important prognostic factor. For
example, the 10 -year cause-specifi c survival for patients with stage
I, II, III, and IV follicular cell type are 68%, 56%, 42%, and 18%,
respectively (Gospodarowicz et al. 1984).
■ “B” symptoms, including unexplained weight loss >10% over 6
months prior to diagnosis, unexplained fever >38°C, and/or
drenching night sweats are associated with poor outcome (Greene et
al. 2002).
■ Other significant prognostic factors include patient age
(younger or older than 60 years), gender (female gender has a better
prognosis in low grade lymphoma), tumor size (less or more than 10
cm in diameter), performance status, level of serum lactate
dehydrogenase (LDH), extent of ex-tranodal involvement, beta-2
microglobulin, and S-phase fraction.
■
The International
Prognostic Index (IPI) for
aggressive NHL includes
five of the abovementioned significant risk
factors to predict overall
survival :
1-stage (I or II vs. III or IV),
2- serum LDH (normal vs.
abnormal), 3-extranodal site
involvement (0 or 1 vs. >1),
4- age of the patient (younger than
60 vs. older than 60),
5- and performance status (ECOG 0
or 1 vs. 2-4).
The IPI risk groups
are determined by the
numerical summation of
the number of adverse
risk factors (0 to 5), and
a higher number of
adverse risk factors are
associated with poor
prognosis
International prognostic
index for aggressive nonHodgkin’s lymphoma
Risk group IPI
score
Low-risk
Lowintermediate
Highintermediate
High-risk
5-Year survival (%)
0–1
2
73%
51%
3
43%
4–5
26%
Prognostic Factors for
HD
The frequency subtypes of HD differs
in different parts of the world. At
present, with effective treatments for
HL, the subtypes are no longer
prognostically relevant. However, some
of these types have particular clinical
features: nodular sclerosis is more
frequent in young women with a large
mediastinal mass. The lymphocytepredominant HL resembles a low-grade,
B-cell lymphoma, and can be treated
with limited irradiation at least in early
stages.
Prognostic factors in HL are age, sex,
stage, and some serum markers such as
sedimentation rate and soluble CD25.
Recently, a prognostic score was
established for advanced HL. This score,
into which seven unfavorable clinical
and laboratory parameters , predicts
treatment failure (low serum albumin,
anemia, male sex, age > 45 yr, stage
IV, leukocytosis, and lymphocytopenia).
Treatment Strategy:
A Role of Surgery : Limited to five clinical situations:
1- Initial diagnosis
P.S.
2- ttt of concurrent unrelated diseases
3- Complications of lymphomas as hypersplenism.
4- Extirpaition of disease involving L.N. as pressure
symptoms related to a localized L.N. enlargement not
responding to local ttt.
5- Management of G.I.T lymphoma (to decrease
incidence of perforation or Hge due to rapid tumour
necrosis after effective chemotherapy.)
B-Role of Radiotherapy:
I- H.D.: Now mainly in the form of involved field radiotherapy to localized
disease or in bulky lymphadenopathy in more advanced stages
High incidence of recurrence after radiotherapy in:
I- IIA with bulky mediastinal disease
2- Extra nodal involvement lEA , IIEA.
3- Mixed cellularity & lymphocytic depletion subtypes.
II- N. H. L.:
* compared to H.D. less firm guid lines for routine Iry radiotherapy
can be provided in PS, I, II N.H.L.
* For localised NHL :PSI, II.
- low grade regional extended radiotherapy (4500
R)
- aggressive radiotherapy + chemotherapy
Lymphatic areas and radiotherapy fields (mantle field, left, and inverted Y with spleen, right).
C-Chemotherapy:
H.D.: the commonest protocoles are:
1- MOPP
2- ABVD:
3-MOPP/ABVD
4-escalated BEACOPP
* chemotherapy is to be given for a minimum 6
monthly cycles at maximally tolerated doses until
achievement complete CR, confirmed by restaging +2
more cycles as consolidation.
TREATMENT OPTIONS AND
RESULTS in HD
. EARLY-STAGE DISEASE (CLINICAL
STAGE I AND II):
extended-field radiotherapy has been
replaced in favor of combined modality
treatment consisting of a short-duration
chemotherapy (e.g., two to four cycles of
ABVD [Adriamycin® (doxorubicin),
bleomycin, vinblastine, and dacarbazine])
followed by involved-field radiotherapy
(20-30 Gy).
. Advanced Stage HD(Clinical Stages III
IV) and
ABVD , The main advantage of ABVD alone is
the relatively low incidence of long-term toxic
effects as compared with alkylating agents-based
regimens.
escalated BEACOPP regimen :
achieved an 87% freedom from progression and a 91%
overall survival after 5 yr. Both schemes are toxic and
therefore should only be administered in larger centers
with much experience and within clinical trials
TREATMENT OPTIONS AND RESULTS
Non-Hodgkin’s Lymphoma
Treatment of Stage I and II Indolent NHL:
Radiation Therapy
■ Radiation therapy is the mainstay treatment of
stage I and II grade I and II follicular lymphoma,
marginal zone lymphoma (non-gastric), and
small lymphocytic lymphoma .
■ IFRT delivers treatment to the
clinically involved region
Treatment of Stage III & IV Indolent Lymphoma
■ Asymptomatic patients with more advanced
stage III or stage IV low-grade NHL can be
closely monitored (watchful waiting) .
■ Rituximab is a “humanized” anti-CD20
monoclonal antibody that can be recommended
for the treatment of indolent non-Hodgkin’s
lymphoma (CD20 positive), and its efficacy in the
treatment of relapsed or refractory indolent NHL
has been repeatedly demonstrated .
■ Combined rituximab and chemotherapy should
be recommended for indolent NHL patients who
have indication for treatment .
.
Treatment of Stage III & IV Indolent Lymphoma
Indications for treatment include:
1- active symptoms
2-cytopenias
3-progression of disease
4- potential organ compromises.
Results from trials comparing R-CHOP
to CHOP and R-CVP to CVP revealed that
overall chemoimmunotherapy appears to
be superior to chemotherapy alone
Treatment of Gastric Mucosa-Associated
Lymphoid Tumors (MALT (:
General Principles:
)
■ For H. Pylori-positive stage IE gastric MALT, antibiotic
treatment of H. Pylori should be used as the initial
treatment . Radiation therapy is an effective modality for
definitive treatment of localized (stage IE or II) gastric
MALT and is recommended for H. Pylori-negative cases,
as well as for patients with deep invasion, active
symptoms, or disease progression after antibiotic
treatment .
■ For stage III or IV gastric MALT, chemotherapy
and/or rituximab should be considered .
Radiation therapy is indicated for local
symptomatic control.
■ Treatment strategy of the more commonly
diagnosed large B-cell lymphoma of the stomach
(comprises approximately 60% of all gastric
lymphoma cases) is identical to that of the
intermediate-grade NHL.
Treatment of Intermediate-Grade (Aggressive)
Non-Hodgkin’s Lymphoma
General Principles:
■ Treatment strategies of the more commonly diagnosed
aggressive NHL, including diffuse large B-cell lymphoma,
grade III follicular lymphoma,peripheral T-cell
lymphoma, and mantle-cell lymphoma, follow similar
recommendations:
■ For stage I and II aggressive NHL, CHOP-based
chemotherapy followed by adjuvant IFRT is the standard
treatment. Rituximab is indicated for CD20-positive largecell non-Hodgkin’s lymphoma .
■ For stage III and IV aggressive NHL, CHOP-based
chemotherapy is the mainstay treatment. Rituximab is
indicated for CD20 positive large-cell non-Hodgkin’s
lymphoma.
COURSE AND PROGNOSIS:
H.D.:
- 10 years actuarial survival has progressively increased from
1% with no therapy to 70% with modern ttt.
N.H.L.:
- Modern chemotherapy progress have revolutionized the
prognosis for many aggressive lymphomas esp., large cell type
and Burkitt’s lymphoma.
Thank you