Management of AF and HF - Belgian Working Group Heart Failure
advertisement

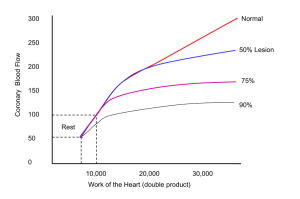
Management of Atrial Fibrillation in Heart Failure Maximo Rivero-Ayerza M.D. Clinical Electrophysiology Ziekenhuis Oost Limburg, Genk Objectives • Assess the relation between AF and HF • Try to establish the optimal treatment strategy Prevalence Unadjusted cumulative incidence of first AF after Heart Failure - Framingham Study ↑ Mortality in AF: - Men HR 1.6 - Women HR 2.7 20% of patients with HF develop AF within 4 years Wang, T. J. et al. Circulation 2003;107:2920-2925 Prevalence Concomitant HF: 13 % age 35 – 64 yrs 21% age > 65 yrs Wattigneyet al. Circulation 2003;108:711-716 Prevalence 0.6 % Patients with Atrial Fibrillation 0.5 0.4 0.3 0.2 0.1 0 D LV O S e Pr S olv Rx II II T A T S T F BI S e I H C F H VC it e El ID V A d on am Di Ge a sic E OP M TI us s en ns o C prevalence increases with severity of heart failure Class I – II Class III - IV Relation between AF and HF Triggers Atrial Fibrillation Substrate AF – Atrial remodeling CHF induced followed by 5 weeks of recovery • Irreversible induction of fibrosis and conduction abnormalities. • Duration of AF was reduced in parallel to LA function. Shinagawa, K. et al. Circulation 2002;105:2672-2678 Effect of intra-atrial pressure on AF 5 cm H2O 18 cm H2O Increases in intra-atrial pressure increases the rate of the dominant frequency at the level of the PV junction compared to LA free wall Kalifa et al. Circulation. 2003;108:668. Effect of intra-atrial pressure on AF Increases in intra-atrial pressure increases the number of waves (rotors) emanating from the PVs Kalifa et al. Circulation. 2003;108:668. Types of AF Triggers ectopic foci Paroxysmal AF Persistent AF Electrophysiologic Remodeling Permanent AF Chronic Substrate fibrosis Stambler et al JCE 2003;14:499 Li, Nattel et al. Circulation. 1999;100:87-95 AF – Hemodynamic Effects *p < 0.01 N=16 NSR AF VVI 60 VVI VVT AVG VVI -AVG VVT Clark DM. JACC 1997; 30:1039-45 Effects of AF in HF Rapid heart rates depress contractility: abnormal force - frequency relationship in heart failure % change in Force 200 Nonfailing Failing 100 0 20 60 120 180 Heart Rate (beats / min) Mulieri Circulation 1992; Effects of AF in HF 344 HF pts FU= 19± 12 months Development of AF (28 pts): • NYHA worsened (2.4 to 2.9) • Peak O2 consumption declined (16 to 11 ml/kg/min) • CI decreased (2.2 to 1.8) • Mitral regurgitation increased (1.8 to 2.4) Pozolli et al. JACC 1998;31(1):197-204. Prognostic significanse of AF CHARM N= 7601 pts (15% with AF) Age= 65 y Baseline AF HR 1.38 (low EF) HR 1.80 (PEF) New onset AF HR 2.57 (PEF) HR 1.85 (low EF) J Am Coll Cardiol 2006;47:1997 Prognostic significanse of AF COMMET N= 3029 pts (20% with AF) Age= 62 y Baseline AF RR=1.29 (univariate) Baseline AF predictive of HF hosp. New Onset AF RR=1.90 (multivariate) Eur Heart J 2005;26:1303 Prognostic significanse of AF DIG N= 6800 pts (11% SVT) Age= 63 y RR= 2.45 CHEST 2000;118:914 Prognostic significanse of AF Epidemiological • As many AF pts developed HF as HF pts developed AF. • New AF in CHF individuals was associated with increased mortality • Antecedent AF was not predictive of mortality in CHF pts. Wang TJ. Et al Circulation. 2003;107:2920 EuroHeart Failure - Mortality P < 0.001 P < 0.001 7% 7% 12 % 13 % In-hospital mortality No AF EHS-HF Previous AF 13 % 19 % 12 week mortality New onset AF Rivero-Ayerza et al. submitted Independent predictors of hospital mortality Multiple logistic regression analysis Less likely to die More likely to die New Onset AF Previous AF Age Male Gender Rapid AF LA Dilatation EF 50% ACS VHD Renal Failure Stroke Elevated BP 0.1 1.5 (1.1-2.0) 1 OR (95%CI) EHS-HF 10 Rivero-Ayerza et al. submitted AF and HF Summary • AF and HF tend to coexist and share predisposing factors • One may directly predispose to the other • The combination of both is believed to carry a worse prognosis then either alone. • In the setting of HF onset of AF seems to be a stronger predictor of adverse outcome irrespective of LV function Management of AF in HF Objectives 1. Prevention of AF would be ideal 2. Avoiding hemodynamic deterioration and improving symptoms 3. Preventing stroke Role of ACEI and ARB’s in prevention of AF 177 pts parox AF End point: recurrence of AF Randomized - Amiodarone (41 % recurrence) - Amio + losartan (19% recurrence) - Amio + perindopril (24 % rec.) Yuehui et al. EHJ 2006;27:1841 ACE inhibition reduces atrial fibrosis in a heart failure model Control 5 Weeks 5 Weeks +Enalapril Li, Nattel, et al Circulation. 2001; 104: 2608 Role of ACEI and ARB’s in prevention of AF • 56,308 patients (11 studies) • Overall RR reduction of 28% • Benefit is similar for ACEI or ARBs • RR reduction 44% in HF Healey J, Baranchuk A, et al JACC 2005;45:1832 Prevention of AF - Statins Recurrence after cardioversion of lone persistent AF Antiinflammatory effect ? / Antioxidant effect ? / Antiarrhythmic effect ? Siu et al. Am J Cardiol 2003; 92:1343 // Shiroshita-Takeshita et al. Circulation. 2004;110:2313-2319. Rate vs Rhythm control Rhythm Control Rate Control • Improve symptoms • Improve symptoms • Improve functional capacity • Avoid side effects of AAD • Lower risk of stroke • Avoid pro-arrhythmia • Avoid anticoagulation •Improve survival Rate vs Rhythm control Vidaillet et al. Curr Opin Cardiol 20:15 // Testa et al. EHJ. 2005 AFFIRM • 4060 patients • No survival benefit (23.8% vs 21.3%) • 23 % Prior HF • Mean EF 55% • Normal EF 74 % NEJM 2002;347:1825 AFFIRM NYHA 6’ walk - SR improved survival - AAD increased (non-cardiac) mortality - Improved FC JACC 2005;46:1891 / NEJM 2002;347:1825 RACE Sub-study HF • Rate control is not inferior to rhythm • If SR is maintained prognosis may improve (more CV death, HF hospitalizations and Bleeding) Hagens et al. Am Heart J 2005;149:1106 DIAMOND • 506 pts with LV dysfunction Survival according to rhythm • Randomized to Dofetilide or Placebo • No effect on mortality • Effect of SR on mortality RR 0.44 (0.30-0.64) Survival according to Rx Pedersen et al. Circulation 2001;104:292 Management of AF in HR SAFE T (persistent AF) CTAF Amiodarone has proven to be safe in HF and CAD patients NEJM 2000;342:913 / NEJM 2005;352:18 Management of AF in HR Fuster, V. et al. Circulation 2006;114:e257-e354 Management of AF in HR In HF patchy fibrosis tends to accumulate at or near PV ostia Jaliffe et al. HRS 2007 AF ablation AF ablation RSPV Management of AF in HF • 58 pts • HF and LVEF <45% • FU= 12±7 m • SR in 69 % at 12 months • LVEF improved 21±13 % • Improved exercise capacity, symptoms, and QOL NEJM 2004:351;23 Relation between AF and HF Ablation Neurohormonal/ Anti-inflammatory Management of AF and HF NYHA II-IV and EF < 35% NYHA I and HF hosp or EF <25% Management of AF in HR Tachycardia Induced Cardiomyopathy - Cardiomyopathy can be caused by any tachycardia (>110 bpm) that occurs as little as 10-15% of day - Severity related to rate and duration of HR - Maximal improvement after rate control may require up to 8 months - After improvement susceptibility to rapid deterioration remains if tachycardia recurs Olshansky et al Circulation 2004 Fenelon et al PACE 1996; 19:95-106 Shinbane J et al. JACC 1997; 29: 709-715 Management of AF in HR AV junction ablation and Pacemaker Implantation Advantages: Rate control without drugs Regularizes ventricular rate Disadvantages Requires permanent pacemaker Fibrillation continues Risk of torsade de pointes Risk of hemodynamic deterioration (RV pacing) Ozcan et al. NEJM 2001;344:1043 Management of AF in HF Favor rhythm control First or infrequent episodes of persistent AF Significant symptoms in AF Difficult rate control Contraindication to long term warfarin Favor rate control Asymptomatic in atrial fibrillation Contraindication to amiodarone Antithrombotic Therapy Risk of stroke 6% / y (5 - 6 fold increase) Warfarin (INR 2.0 - 2.6): 62% reduction (CI 48% - 72%) 37 NNT to prevent 1 stroke major hemorrhage: 0.6% / yr 20% discontinue anticoagulation Aspirin (25 mg - 1300 mg/day) 22% reduction (2% - 38%) Hart et al. Ann Intern Med 1999;131:492 Antithrombotic Therapy CHADS² CHADS Stroke rate Score 1 2.8 %/y Score 2 4.0 %/y Score 3 5.9 %/y Score 4 8.5 %/y • Diabetes Score 5 12.5 %/y • Previos stroke (2 points) Score 6 18.2 %/y • Congestive HF • Hypertension • Age >75 Gage et al. JAMA 2001;285:2864 Summary • AF and HF are not only clinically associated but are physiopatologically inter-related • AF seems to be a prognostic indicator (certainly recent onset AF) irrespective of LV performance. • Consequently prevention of AF should carry a better prognosis • Although no benefit of rhythm vs rate control has been shown. Data suggest that certain subgroup of patients will benefit from SR • Irrespective of management strategy, antithrombotic Rx is warranted Conclusion “I have been poor and I have been rich. Rich is better.” Attributed to Sophie Tucker