Incisions in cardiothoracic surgery

IN THE NAME OF GOD
Dr.mehdi hadadzadeh
Assistant professore of cardiovascular surgery
A surgical incision opens an aperture into the thorax to permit the work of the planned operation to proceed
If an operation is difficult, you are not doing it properly," applies directly to the incision used
The choice of incision :
underlying pathology
the site (e.g. lung, chest wall, oesophagus)
experience of the surgeon
Types of incisions
Median Sternotomy
Posterolateral thoracotomy
Anterolateral thoracotomy
Lateral thoracotomy
Bilateral thoracosternotomy
Subxiphoid(pericardial window)
Posterolateral thoracotomy
gold standard of thoracic incisions
excellent exposure for most general thoracic procedures including the lung, heart, aorta, the lower esophagus, and diaphragm
This approach is also used for spinal operations
Preoperative preparation
Assessment of pulmonary function
given a dose of antibiotics preoperatively
preoperative education and incentive spirometry training as to the importance of adequate inspiration postoperatively to prevent atelectasis (lung collapse
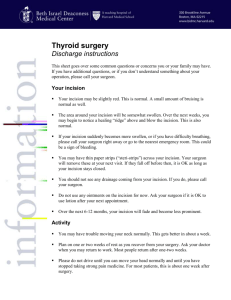
Position
complete lateral decubitus position
use of sandbags, rolled sheets front and back or bean bags supporting the back and the abdomen
The lower leg is flexed at the knee and hip while the upper leg lies straight on the top of the pillow
to avoid post operative complications ;
cutaneous necrosis,
venous thrombosis
or nerve compression.
arm placed on an angle pad
free from any fixation.
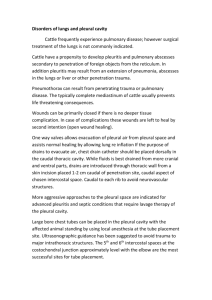
Incision
The position of the vertebral spines and the nipple is notified.
The standard incision follows between scapula and mid-spinal line to the anterior axillary line
passing 3cm below the tip of the scapula.
The skin incision :No. 10 scalpel
latissimus dorsi and serratus anterior muscles : No. 10 scalpel or cautery
Posteriorly, the muscle layers of the rhomboid and trapezius are incised
The pleural space :incising the musculature between the ribs or via an osteotomy
transect the muscles on the superior border of the ribs to avoid injuring the neurovascular bundle.
ribs may be transected or resected
at the level of the 5th rib for exposure of the upper thoracic area :COA
level of the 6th or 7th rib for lower thoracic area (e.g., lower esophageal or diaphragmatic surgery)
After operation drainage tubes must be placed
The rib approximator is closed and No.1 chromic or No. 1 vicryl sutures are placed to encircle the bone along the length of the incision.
Silk sutures are to be avoided as it increases postoperative pain
The cut ends of the trapezius and latissimus dorsi muscles are then approximated and sutured subcutaneous tissue is closed using an interrupted 3-0 absorbable sutures.
The skin is closed using surgical clips or a running 4-0 subcuticular stitch such as Monocryl.
disadvantages of this incision
increased potential for blood loss and moderate time requirement for opening and closing the incision
prolonged ipsilateral shoulder and arm dysfunctions
compromised pulmonary function and chronic post thoracotomy pain syndromes
scolioses have been described in children
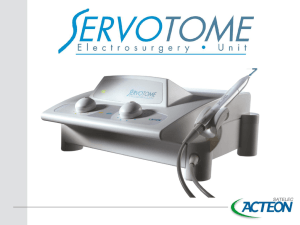
Median sternotomy
Most common thoracic incision
Indications:cardiac operations-anterior mediastinal lesions-bilateral lung procedures
Speed in opening and closing
Supine position and arms in patient,s side
Incision
Incision from below the suprasternal notch toa point between the xyphoid and umblicus
An electric saw with a vertical blade is used
An oscillating saw is used for repeated sternotpmy
Bone wax is a useful tool to control bleeding from sternum
sterile mixture of beeswax and isopropyl palmitate
Sternal retractor is used in lower thired of the sternum and gradually opened
Stainless steel wire is at present the standard suture in median sternotomy
Disadvantage of this incision
Scar formation
Brachial plexus injury
Chronic chest pain
Axillary(lateral)thoracotomy
Advantages:muscle sparing-ease and speed-good cosmetic
Disadvantages:limited exposure
Choice in majority of pulmonary resections ,PDA ligation,PA banding and….
Lateral decubitus position homolateral arm is abducted at
90° at the shoulder level, flexed at the elbow
Incision Between posterior border of pectoralis major and anterior border of latisimus dorsi
through the 4th or 5th intercostal space;
Bilateral
thoracosternotomy(clamshell)
Previously choice for bilateral lung transplant
Incision along the inframammary creases and across the sternum
4 or 5 th intercostal space
Poor healing of wound
Anterolateral thoracotomy
Useful in variety of operation on heart,pulmonary resection and esophagus
Supine and operation site elevated30 degree
Incision from lateral border of sternum to midaxillary at 4or5interspace
Pectoralis major and seratus anterior is divided
Subxiphoid incision(pericardial window)
Indications:pericardial effusion,pericardial biopsy,epicardial pacemaker
Supine posision,midline incision over the xiphoid
Intrapleural(chest) tubes
Whenever thoracotomy has been done
exit of fluids and air and monitors of bloodloss
Separate incision