File - Matt genther

COPD v. Asthma
MATT GENTHER
COPD
Chronic Obstructive Pulmonary Disease (COPD)
Chronic bronchitis and Emphysema
Two forms of COPD with specific pathologic lung changes
Progressive irreversible airflow limitation
Associated with abnormal inflammatory lung response (McCance &
Huether, 2010)
COPD
Tobacco smoke is the most common cause of COPD
Other causes include
Air pollutants, genetic factors, respiratory infections and occupational exposures (Postma, et al., 2014).
COPD is the third leading cause of death in the United states
12-16 million Americans report to have been diagnosed (Kim & Criner,
2013)
Most common to report
Age 65+, current and former smokers, women, hx of asthma, people with low incomes and individuals with less than high school income
(McCance and Huether, 2010)
COPD – Chronic Bronchitis
Defined as being associated with chronic cough and sputum production
At least 3 months per year for 2 consecutive years
With increased exacerbation rate and accelerated decrease in lung function (Kim & Criner, 2013)
Chronic Bronchitis (CB) primary risk factor is smoking (42%) but can be found in 4-22% of non-smokers (Kim & Criner, 2013)
Potential risk factors include inhalation of biomass fuels, dust, and chemical fumes.
COPD – Chronic Bronchitis
Epidemiology of CB, high prevalence of patients with COPD
14-76% of all patients with COPD
10 million people in the US
Majority between 44-65 years of age (Kim & Criner, 2013)
Image (Buggy, 2007)
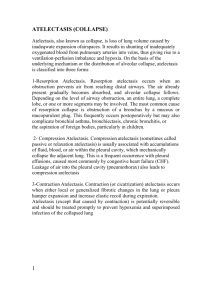
COPD – Chronic Bronchitis
Inspired irritants increase mucous and number of goblet cells in airway
Creating thicker secretions
Increased mucous promotes bacterial cell growth
Embedded secretions impair airway function
Bronchial walls become inflamed leading to wall narrowing and bronchospasm (McCance & Huether, 2010)
Initially only the large bronchi are affected though all airways are involved
Obstruction greater on expiration
Profusion mismatch traps gas in distal lungs
Decrease tidal volume, hypoventilation, and hypercapnia (McCance &
Huether, 2010)
COPD – Chronic Bronchitis
Clinical manifestations:
Decreased exercise tolerance, wheezing, shortness of breath
Productive cough, frequent pulmonary infections, and copious thick sputum production.
(McCance & Huether, 2010)
Forced expiratory volume (FEV1) and forced vital capacity (FVC) are declined in CB
Image (Kim & Criner, 2013)
COPD – Chronic Bronchitis
Diagnosis is based on a history of symptoms, physical exam, chest radiography and blood gas analysis (McCance & Huether, 2010)
Prevention is the best treatment because damage is irreversible
Smoking cessation before the damage is great is a mainline defense
Decreases goblet cell hyperplasia (Kim & Criner, 2013)
Antibiotics, mucolytics, corticosteroids, oxygen therapy and bronchodilators are first line medications for CB
Reduction of exacerbations, increase lung function and decreasing the infectious and inflammatory response of the body are the mechanisms of treatment (Poole, Black & Cates, 2012)
COPD Emphysema
Emphysema is characterized by destruction of alveolar walls and enlargement of gas exchange airways
(acini)
Elastic recoil is lost due to aging
Most likely cause of emphysema before old age is secondary to smoking
(McCance & Huether, 2010)
COPD – Emphysema
Three classifications of Emphysema: Panacinar, Parasceptal and
Centroacinar.
Panacinar emphysema destroys entire alveolus uniformly, mostly found in lower lungs
Parasceptal emphysema involves alveolar ducts and sacs in the peripheral lung
Centroacinar emphysema starts in the bronchioles and spreads towards the periphery (Higginson, 2010)
COPD – Emphysema
1-2% of cases are due to a lack of alpha-1 antitrypsin, in which alveoli lose elasticity
More commonly, noxious stimuli inhalation leads to emphysema
Cigarette smoke is the most common causing inflammatory response
Neutrophils, macrophages and lymphocytes produce chemicals that decrease the elasticity in cells, creating fewer larger alveoli (Higginson,
2010)
Inhaled toxins and air pollutants also know to cause emphysema
COPD – Emphysema
Emphysema is a progressive nonreversible disease of the alveoli
Hypoxemia causes the lungs to go through pulmonary hypoxic vasoconstriction
The constriction leads to pulmonary hypertension and eventual right sided heart failure, cor pulmonale (Higginson, 2010)
COPD – Emphysema
Clinical manifestations:
Dyspnea upon exertion and at rest, some unproductive coughing, thin stature and prolonged expiration
Barrel chest, hyperresonant percussion, pursed lip breathing and tripod breathing positioning (McCance & Huether 2010)
Diagnosis is based on respiratory signs and symptoms
Pulmonary function test
Size and shape of chest, breathing pattern, shortness of breath, clubbing of fingers, auscultation and percussion
X-ray, CT scans, arterial blood gases and EKG (Bailey, 2012)
COPD - Emphysema
Smoking cessation primary mechanism to stop damage of emphysema
Oxygen therapy, pulmonary rehab, bronchodilators, corticosteroids, and surgery used to treat disease
Disease is irreversible
Treatments used to reduce symptoms, dyspnea and hypoventilation
Asthma
Chronic disorder of the airway, involving interactions of airway obstruction, bronchial hyperresponsiveness and inflammation
(McCance and Huether, 2010)
This heterogeneous syndrome affects 300 million individuals worldwide
Airways suffer from chronic inflammation and small bronchial diameter
(Aguilar, Walgama & Ryan, 2014)
Asthma
Asthma occurs at all ages, half of all cases are found in children
Familial disorder linking over 100 genes with susceptibility
Eosinophils, mast cells, leukotrienes, and bronchial hyperresponsiveness increase the production of IgE
IgE plays a role in hypersensitivity and allergic response (Aguilar,
Walgama & Ryan, 2014)
Risk factors: family history, exposure to pollutants and smoking, respiratory viral infections, and obesity (McCance & Huether, 2010)
Prevention and treatment of allergic rhinitis may prevent asthma
(McCance & Huether, 2010)
Asthma
Inflammation causes wheezing, breathlessness, chest tightness and coughing
Most often at night or early morning
Episodes are widespread in lungs, resolve either spontaneously or with treatment (Postma, et al., 2014)
Expiratory flow is decreased by airway obstruction causing air trapping
Decreased alveolar perfusion causes hypoxia and respiratory acidosis and can lead to respiratory failure (McCance & Huether,
2010)
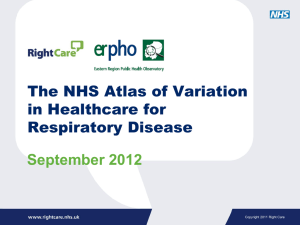
Asthma
Host factors
Perinatal factors
Childhood exposures
Adult exposures
Male sex in childhood, female sex in adulthood
(Family) history of asthma
Genetic constitution
Airway hyperresponsiveness
Atopy
Low lung function
Overweight
Maternal smoking
Maternal diet
Mode of delivery
Viral respiratory infections
No breastfeeding
Microbial deprivation
Family history of COPD
Family history asthma/atopy
Genetic constitution
Airway hyperresponsiveness
—
Low lung function
—
Maternal smoking
—
—
Respiratory tract infections
—
Maternal smoking
Environmental tobacco smoke exposure Indoor air pollution
Air pollution
Occupational exposures
Cigarette smoking
Outdoor air pollution
—
—
Occupational exposures
Cigarette smoking
Outdoor air pollution
Indoor air pollution
Asthma
Pulmonary function tests are normal in between exacerbations
During attacks chest constricts, expiratory wheeze is present, dyspnea, coughing, tachycardia, prolonged expiration, and tachypnea
Prolonged bronchospasm can lead to status asthmaticus
Acidosis can follow PACO2 rises and can cause sudden death
(McCance & Huether, 2010)
Asthma
Diagnosis based on attacks, family history, allergies and an decreased FEV1, FVC and total lung capacity
Classified by severity: intermittent, mild persistent, moderate persistent and severe consistent (McCance & Huether, 2010)
Treatment includes avoiding allergens, short acting beta agonist inhalers for acute exacerbations, anti-inflammatory medications, and corticosteroids (Postma, et al., 2014)
COPD v. Asthma: Study Questions
1.
2.
Which form of emphysema damages the entire acinus and tends to not be associated with smoking?
a.
b.
Centriacinar emphysema
Panacinar emphysema c.
d.
Paraseptal emphysema
Cor pulmonale
Which cells are NOT associated with inflammation and destruction of alveolar elasticity?
a.
b.
c.
d.
Neutrophils
Macrophages
Fibroblasts
Lymphocytes
COPD v. Asthma: Study Questions
3.
4.
5.
Increased mucous production found in CB is associated with?
a.
Goblet cell hyperplasia b.
c.
Inflammatory cytokines
Pneumonia d.
Hypoventilation
Which group has a decreased risk for asthma?
a.
b.
Children of parents that smoke
Children living in cities c.
d.
Children with many allergies
Children that live in rural areas
Pulmonary hypertension causes?
a.
b.
Left sided heart failure
Right sided heart failure c.
d.
Diabetes
Tuberculosis
References
Aguilar, P., Walgama, E., & Ryan, M. (2014). Other asthma considerations. Otolaryngologic Clinics Of North America, 47(1), 147-
160. doi:10.1016/j.otc.2013.08.015
Bailey, K. (2012). The Importance of the Assessment of Pulmonary
Function in COPD. Medical Clinics Of North America, 96(4), 745-752.
Buggey, T. (2007). Storyboard for Ivan's morning routine.
Diagram. Journal of Positive Behavior Interventions, 9(3), 151. Retrieved
December 14, 2007, from Academic Search Premier database
Hadjiliadis, D. (2011). Emphysema. Retrieved from http://www.nlm.nih.gov/medlineplus/ency/imagepages/17055.htm
Hadjiliadis, D. (2011). Cor pulmonale. Retrieved from http://www.nlm.nih.gov/medlineplus/ency/imagepages/17055.htm
Higginson, R. (2010). COPD: pathophysiology and treatment. Nurse
Prescribing, 8(3), 102-110.
References
Kim, V., & Criner, G. (2013). Chronic bronchitis and chronic obstructive pulmonary disease. American Journal Of Respiratory & Critical Care
Medicine, 187(3), 228-237. doi:10.1164/rccm.201210-1843CI
McCance, K., & Huether, S. (2010). Alterations of Pulmonary Function.
In Pathophysiology: The biologic basis for disease in adults and
children (6th ed., pp. 1266-1309). Maryland Heights, Mo.: Mosby Elsevier
Poole, P., Black, P., & Cates, C. (2012). Mucolytic agents for chronic bronchitis or chronic obstructive pulmonary disease. Cochrane
Database Of Systematic Reviews, (8), doi:10.1002/14651858.CD001287.pub2
Postma, D., Reddel, H., ten Hacken, N., & van den Berge, M. (2014).
Asthma and chronic obstructive pulmonary disease: similarities and differences. Clinics In Chest Medicine, 35(1), 143-156. doi:10.1016/j.ccm.2013.09.010