Dr Robert Wilder 2114 - Richmond Endurance Athlete Symposium
advertisement

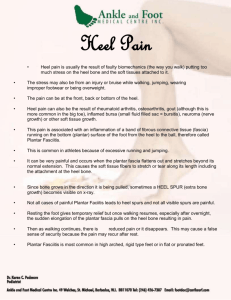
Common Running Injuries Robert P. Wilder, MD, FACSM Chair, Physical Medicine & Rehabilitation The University of Virginia Medical Director, The Runner’s Clinic at UVA Team Physician, Ragged Mountain Racing Objectives • Identify common contributors to running injuries • Describe treatment for heel pain, stress fractures, and patellofemoral pain syndrome • Understand the importance of proper mechanics in managing injury • Outline criteria for running while treating injury Epidemiology of Running Injuries 30 million active runners 70% all runners sustain significant injury 40% knee 15% each: shin, achilles, hip/groin 10% foot and ankle 5% spine 25% recreational 5% elite Epidemiology of Running Injuries 4% bit by dogs 0.3% hit by bicycles 0.6% hit by cars 7% hit by thrown objects Principle of Transition “Culprits & Victims” Intrinsic Abnormalities Malalignment Muscle imbalance Inflexibility Muscle weakness Instability Extrinsic Abnormalities Training errors Equipment Environment Technique Sport-imposed deficiencies Examination of the Injured Runner History Biomechanical assessment Site-specific exam Dynamic exam Shoe exam Ancillary testing radiologic electrodiagnostic compartment testing History • • • • • • • • • • • • Prior injury history Team/Club Identify transitions MPW (20, 40) Long run (< 1/3 weekly total) Intensity Surface (? Muscle tuning) Shoes/orthotics (350-400 miles) Cross Training Goals Life Stressors/fatigue Females: eat d/o, menstrual irreg, osteopenia Physical Examination • • • • • Biomechanical assessment Site specific examination Dynamic examination Ancillary testing Shoe examination Functional Screening • • • • • • • Single Leg Stance Single Leg Squat Bilateral Squat FHB isolation Step-down Test STAR Excursion Test Swing Test Functional Screening Single Leg Stance Functional Screening Single Leg Squat Functional Screening Bilateral Leg Squat Functional Screening FHB Isolation Functional Screening Step-Down Test Functional Screening STAR Excursion Test Functional Screening Swing Test Heel Pain in Runners Plantar Fasciitis • 10% U.S. Population • 600,000 outpatient visits annually • 7-9% all running injuries Plantar Fascia • Thick aponeurosis • Arises from medial calcaneal tuberosity • Spans arch • Bands circle flexor tendons • Insert proximal phalanx Functions During Gait Cycle • Heel strike: Allows midfoot to become flexible, absorb shock, conform to uneven surface • Toe off: Windlass Mechanism: Shortening increases arch, locks midtarsal, stabilizes toe off Pathophysiology • Overuse • Inflammation • Chronic changes (collagen necrosis, angiofibroplastic hyperplasia, chondroid metaplasia, matrix calcification) • Tearing • Medial vulnerable (thin, limited vascular supply, limited ability to stretch Risk Factors • • • • • • • • Obesity Excessive time on feet Limited ankle motion (tibiotalar) Limited great toe mobility (extension) Inflexibility (HS and achilles) Pes cavus Pes planus Leg length inequality (short leg) Presentation • • • • Plantar heel pain A.M. pain Mid arch (sprinters) Increased pain with running • Imaging primarily to rule out other causes Treatment • • • • Relative Activity Modification Anti-inflammatories Flexibility (HS, gastroc-soleus, plantar fascia) Manual therapy (ankle and great toe mobility: tibiotalar subtalar, great toe) • Strength (Foot intrinsics, ankle stability, lower quarter stability) Treatment (cont) • • • • • Devices – CTF brace, heel cushions Low dye taping Night splints and socks Inserts Steroid injections Treatment (cont) • • • • • ESWT (> 12 mos) Botulinum A Autologous blood PRP Prolotherapy Recalcitrant Cases • Confirm diagnosis • Surgical release – 75-95% “some improvement” – 27% significant pain – 20% activity restriction • • • • Fasciectomy + neurolysis of nerve to ADM Percutaneous plantar fasciotomy Flouroscopically-assisted fasciotomy US guided fasciotomy Heel Pain Differential • Fat Pad Insufficiency • Calcaneal Stress Fracture Heel Pain Differential (cont) • Neuropathies – Tarsal Tunnel Syndrome – Medial plantar nerve (“Joggers Foot”) – First Branch, Lateral Plantar nerve (“Baxter’s Neuropathy”) – Radiculopathy Heel Pain Differential (cont) • Tendonopathies – PTTD (posterior tibial) – Flexor – Peroneal – Achilles Heel Pain Differential (cont) • Spring Ligament injury Heel Pain Differential (cont) • Bursitis – Pre-achilles – Retrocalcaneal Heel Pain Differential (cont) • OS Trigonum Syndrome (differentiate from posterior talus fracture) Heel Pain Differential (cont) • Haglund’s Heel Pain Differential (cont) • Sever’s Syndrome (kids) Heel Pain Differential (cont) • Achilles enthesopathy (consider inflammatory) Heel Pain Differential (cont) • Tarsal coalition Heel Pain Considerations • • • • Ankle mobility (tibiotalar, subtalar great toe) Flexibility (HS, GS, PF) Ankle stability Lower quarter stability Stress Fractures Failure of bone to adapt adequately to mechanical loads (ground reaction forces and muscle contraction) experienced during physical activity 1. 2. 3. 4. Tibia Metatarsals Fibula Navicular Stress Fractures - Pathophysiology Stress Fractures (cont) • Non-critical (relative rest 6-8 wks) • Medial tibia • Metatarsals 2,3,4 Stress Fractures (cont) At risk fractures: – Femoral neck – Anterior tibia – Medial malleolus – Navicular – Base 5th metatarsal Femoral Neck Superior (distraction) – higher incidence worsening/ non union Inferior – (compression) Anterior Tibia Casting vs relative rest up to 6-8 months If no healing – ortho (transverse drilling, grafting, medullary fixation) Navicular • Tender N-spot • Critical zone middle 1/3 • Non-weight bearing 6-8 weeks • Progressive activity over 6 more weeks Proximal 5th Metatarsal • • • • Jones fx of proximal diaphysis Cast 6-10 weeks Non-union: ortho Consider ortho early in competitive • Contrast with avulsion: symptomatic RX Patellofemoral Syndrome • Pain associated with the articular surface of the patella and femoral condyles, its alignment and motion • “Runners Knee” #1 presenting complaint to Runner’s Clinics • #1 cause lost time in basic training military recruits PFS - Classification • Patellofemoral instability • PFS with malalignment • PFS without malalignment PFS – Contributing Factors • Bony abnormalities • Malalignment • Soft tissue abnormalities PFS – Bony Abnormalities • Dysplasia of femur • Asymetry of patellar facets PFS – Lower Extremity Malalignment • • • • • • • • Femoral anteversion Increased Q angle Knee valgus (knock kneed) Lateral patellar tilt Lateral tibial tuberosity Abnormal tibial torsion Hyperpronation Restricted dorsiflexion PFS – Muscle/Soft Tissue Imbalances • • • • Weak, delayed activation VMO Weak quads Tightness Quads, ITB, hamstring, gastroc Weak hip muscles , abductors, gluts Patellofemoral Syndrome - Diagnosis • • • • • • Anterior, peripatellar, subpatellar pain Downhill and downstairs Theater sign Contributing factors Apprehension (shrug) sign X-ray Patellofemoral Syndrome - Treatment • • • • • • Correct the functional deficits! Bracing, taping Foam roller Correct pronation (if excessive) Adjust training – avoid hills, bike mod Correct the functional deficits! Shoes • • • • • • • Lots of options (a good thing) Can affect impact forces, loading rates, torque forces ? Relation to shoes, form or both Rarely does “one size fit all” If it ain’t broke, don’t fix it? All transitions gradual With barefoot, minimalist ensure stability and form cues • • • • Cross train (aqua run, eliptical bike) Walk, then walk – jog, then run 10% per week rule Long run increases no more than 2 miles Relative Activity Modification Guidelines Rule #1 • If you feel mild pain (0-3/10): it is OK to run • If you feel moderate pain (4-6/10): reduce activity until pain level is mild. • Severe pain (> 7/10): no running Relative Activity Modification Guidelines Rule #2 • Pain that decreases with activity is OK. • Pain that gets worse with activity is bad; time to reduce or stop activity. Relative Activity Modification Guidelines Rule #3 • No limping allowed. • If the pain alters your gait pattern, it is time to reduce or stop the activity until you have normal biomechanics.