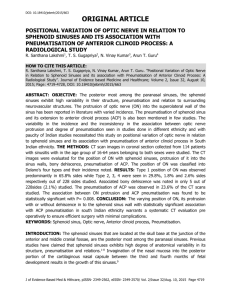
192_eposter - Stanley Radiology
advertisement

Abstract Id: IRIA-1173 Anatomy: * Maxillary sinus * Frontal sinus * Ethmoid sinus * Sphenoid sinus Sphenoid sinus: It spreads laterally to invade the greater and lesser wings and medial & lateral pterygoid plates of sphenoid. A foramen in the center of each turbinate allows the sinus of each side to communicate with the nasal cavity at the sphenoethmoidal recess. Recently transsphenoidal hypophysectomy is done and has significant advantages over open craniotomy. Types of sphenoid sinus - 1.Conchal 2.Pre sellar 3. Sellar. Conchal Pre sellar Relationship of important structures: Optic nerve- superior – lateral Carotid canal / cavernous sinus- mid- lateral Vidian nerve / maxillary nerve – inferior - lateral Sellar Frontal recess: It is the bordering anatomical structure forming the walls of the passage from frontal sinus to the middle meatus. Boundaries- Anteriorly by the agger nasi cells, laterally by orbit, medially by middle turbinate and posteriorly by bulla lamella. * Bent’s classification of frontal cell variants: Type I- Single frontal recess cell above the agger. Type II-Tier of air cells above agger projecting in to frontal recess. Type III- Single massive air cell above agger expanding into frontal sinus. Type IV- single isolated cell within frontal sinus. * Middle turbinate: It lies inferomedial to the anterior ethmoidal air cells.Middle turbinate also serves as a important surgical landmark for skull base, frontal sinus and orbit. • Anterior- oriented in sagittal plane and it is vertically attached to the cribriform plate. • Middle- oriented in frontal plane and it is attached to the lamina papyracea or basal lamella laterally. It separates anterior and posterior ethmoids. • Posterior-oreinted in horizontal plane and it is attched to the perpendicular plate of palate. * Anterior osteomeatal unit: It is a complex anatomic region at crossroads of mucociliary drainage from frontal, anterior and maxillary sinuses. Components of anterior osteomeatal unit are: • Maxillary ostiummaxillary sinus. drainage channel of • Infundibulum- common channel that drains the ostia of maxillary & ethmid sinuses to the hiatus semilunaris. • Uncinate process- hook like process that arises from posteromedial aspect of nasolacrimal duct and froms the anterior boundary for hiatus semilunaris. • Ethmoid bulla- usually a single air that projects inferomedially over hiatus semilunaris. • Hiatus semilunaris -final drainage passage; region that between ethmoid bulla superiorly and free edge of uncinate process. It can be demonstrated in saggital section of CT. *Posterior osteomeatal unit: It comprises of postero superior concha(sphenoethmoid recess), which is draining site for sphenoid sinus through sphenoid ostium. Inferior to superior concha in the superior meatus, there are two opening for posterior ethmoidal air cells. Sagittal CT image showing sphenoid ostium & sphenoethmoid recess * UNCINATE PROCESS: • The uncinate process is a superior extension of the lateral nasal wall that is anatomically relevant for draining frontal recess. • Variations such as hypertrophy, deviation and pneumatization may affect the drainage, generating abnormalities in osteomeatal complex. Horizontal uncinate Pneumatisation of uncinate Vertical uncinate Hypertrophy of uncinate * OLFACTORY FOSSA: It is a variable depression seen in cribriform plate that medially bounded by perpendicular plate and laterally by lateral lamella. KEROS CLASSICIFICATION: The depth of olfactory fossa is determined by the height of the lateral lamella of cribriform plate by Keros in 1962 in to three catergories. Type III essentially expose the thin cribriform plate to potential damage from trauma, tumour erosion, local nasal surgeries and orbital decompression. Type I- 1-3mm. Type II- 4-7mm. Type III- 8-16mm. Type I Type II Type III Anterior ethmoid foramen: It as a small opening in the ethmoid bone and transmits the anterior ethmoid artery and nerve. Importance- It is the anatomical border for anterior and posterior ethmoid air cells in coronal plane. Coronal CT image showing anterior ethmoid foramen * STRUCTURES DEMONSTRATED BETTER IN SAGITTAL SECTION CT: • Hiatus semilunaris • Frontal recess • Spheno ethmoid recess • Type of sphenoid sinus • Agger nasi cells Computed tomography(CT): It is the imaging modality of choice for assessment of paranasal sinus. A complete coronal and axial sections CT scan series provides an excellent and comprehensive evaluation of PNS. CT excels over MRI at evaluating fine bone details, assessment of fibro-osseous lesions of PNS and sino facial lesions. CT plays an important role in the pre-operative evaluation of patients and provides a “ROAD MAP” to guide the surgeons during surgery. PIT FALLS IN CT: • Due to its complex projections, artefacts induced by very high density structures around PNS, by the patient movement, limited soft tissue resolution and even radiation exposure in CT examinations limits frequent usage in children and pregnant women. • For these reasons, MRI is considered as imaging modality in conditions. • Anatomical variations are which impairs the normal functional drainage pathways and increase the risk of surgeries. • Identification of these anatomic variants of paranasal sinus helps the surgeons to access sites of diseases which are extremely difficult. * Agger nasi cells (ANC): It is the most constant and anterior of ethmoid air cells. It is located anterior to the vertical attachment of middle turbinate to the skull base. Agger nasi cells seen in axial and coronal CT Spheno ethmoid cells (Onodi cell): This is formed by lateral and posterior pneumatization of the most posterior ethmoid cells over the sphenoid sinus . The presence of Onodi cells increases the chance that the optic nerve and carotid artery would be exposed in the pneumatized cell. Infra orbital air cells(Haller Cells): These are centered inferior to the ethmoidal bulla and grow into the floor of the orbit. They may narrow the maxillary sinus ostium, especially if infected. Axial and Coronal sections CT images showing Haller cells Ethmoidal Bulla: The Ethmoidal bulla is an anterior ethmoidal air cell of variable size located just posterior to the free edge of the uncinate process. An enlarged ethmoidal bulla may compromise the outflow of both the maxillary antrum and the frontal sinus by distorting the ethmoid infundibulum or hiatussemilunaris and the frontal recess. Deviated nasal septum (DNS): The nasal septum may be focally deviated inferiorly at the chondrovomeral junction or have a more broad based curvature . Septal spurs may be associated with septal deviation, which makes surgical access difficult and narrow the middle meatus or Ethmoid infundibulum. Coronal section CT image showing nasal septum deviation towards right side Concha Bullosa: It is the pneumatization of the inferior bulbous portion of the turbinate. A large concha bullosa, which usually present with septal deviation may obstruct the drainage pathway of the antrum by distorting the uncinate process and narrowing the infundibulum. Paradoxical middle turbinate turn: The middle turbinate may have a lateral convexity ( a paradoxical turn). If large, it is associated with septal deviation and may impair access to the osteo- meatal unit. Coronal CT image showing paradoxical turn of middle turbinate Maxillary sinus septations: The maxillary sinus septum may be fibrous or bony and often extends from the infra orbital canal to the lateral wall. If not recognised, it may lead to inadequate drainage of the antrum. SPHENOID SINUS SEPTATION: It is the presence of multiple septation within the sphenoid than the main septa. It is percepted that multiple accessory septs are seen more commonly on the right side of main septa. It makes the access difficult for the surgeons while performing surgeries invloving transsphenoidal approach. axial section CT showing multiple septa sphenoid sinus CLOSE Technique: C- Cribriform • Assess the keros type. • Look for assymmetry. L- Lamina Papyracea • Check for dehiscence or pathologic fractures. O- Orbit, Optic nerve, Onodi cells • Check for dehiscence . • Assess for onodi cells (superior-lateral to sphenoid). • Orbital slope. S – Sphenoid, Skull base • Assess for carotid dehiscence and aeration patterns. • Conchal, Pre-sellar & Sellar(thickness of clivus). • Assess slope of skull base. • Assess if roof of sphenoid is level with skull base. E- Ethmoid arteries. • CT is a sensitive technique for evaluating para nasal sinus. • Identification of anatomical variants are important because, it helps surgeons during sinonasal surgeries. • CT helps in staging the PNS diseases by its extension and involvement of surrounding structure. 1. 2. 3. 4. Scuderi A J, Harnsberger H R, Boyer R S. Pneumatization of the paranasal sinuses: normal features of importance to the accurate interpretation of CT scans and MR images. AJR Am J Roentgenol. 1993;160:1101–1104. Sirikci A, Bayazit Y A, Bayram M, Mumbuc S, Gungor K, Kanlikama M. Variations of sphenoid and related structures. Eur Radiol. 2000;10:844–848. Ariji Y., Ariji E., Yoshiura K., Kanda S. 1996. Computed tomographic indices for maxillary sinus size in comparison with the sinus volume. Dentomaxillofac. Radiol. 25: 19–24. Bolger WE, Butzin CA, Parsons DS. Paranasal sinus- Bony anatomic variation and mucosal abnormalities : CT analysis for endoscopic sinus surgery Laryngoscope Jan 1991; 101:56-65.