糖尿病治療の新たな選択
~なぜ私はピオグリタゾンを使のか~
糖尿病学術講演会
~ピオグリタゾン15周年を記念して~
座長 埼玉医科大学かわごえクリニック 病院長 片山 茂裕先生
2015年2月2日(月) 19:30-21:15
川越プリンスホテル
埼玉県川越市新富町1-22 Tel.(049)227-1111
埼玉医科大学 総合医療センター 内分泌・糖尿病内科
Department of Endocrinology and Diabetes,
Saitama Medical Center, Saitama Medical University
松田 昌文
Matsuda, Masafumi
主催 武田薬品工業株式会社 後援: 川越市医師会
Conflict of interest
発表者名:松田
昌文
演題発表に関連し、開示すべきCOI関係にある企
業などはありません。
当糖尿病学術講演会は武田薬品工業(株)の主
催、川越市医師会の後援で行われます。
経口血糖降下薬による寛
肥満(メタボ)2型糖尿病治療の戦略
解導入(糖毒性解除)主
にSU薬の導入と減量に
薬物療法の実践
ついて(1章 血糖降下薬
治療の実際)
谷澤幸生
山口大学大学院医学系研究科
病態制御内科学教授
経口血糖降下薬による維
持療法 インスリン分泌系
薬物と抵抗性改善薬の組
合せなど(1章 血糖降下
薬治療の実際)
松田昌文
埼玉医科大学総合医療センター
内分泌・糖尿病内科教授
糖尿病に対する介入
低血糖を避け,膵β細胞機能を維持し
合併症の発症や進展を抑制する
食事療法
運動療法
インスリン分泌させる
治療ではない!
糖尿病の治療の基本は
膵島(膵β細胞)保護!
= パラダイムシフト
なるべく早期からの薬物介入も辞さない
• 血糖管理 低血糖なしに
• 体重管理
• 血圧・血中脂質管理
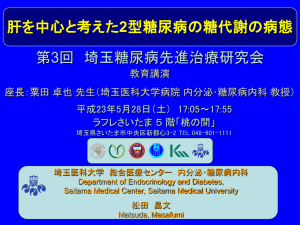
低血糖の発生頻度と認知症
人数 (%)
痴呆あり
痴呆なし
(n=1822)
(n=14845)
全ての低血糖
No
Yes
低血糖の回数
0回
1回
2回
3 回以上
年齢調整罹患率
/1万人・年
(95% CI)
オッズ比
リスク/年, %
(95% CI)a
1572 (10.34)
250 (16..95)
13630 (89.66)
1215 (83.05)b
327.60 (311.02-343.18)
566.82 (496.52-637.48)
2.39 (1.72-3.01)
1572 (10.34)
150 (14.84)
57 (22.26)
43 (20.40)
13630 (89.66)
852 (85.16)
201 (77.74)
162 (79.60)b
327.60 (311.02-343.18)
491.73 (412.60-570.80)
761.75 (561.24-962.27)
755.46 (526.46-984.46)
1.64 (0.91-2.36)
4.34 (2.36-6.32)
4.28 (2.10-6.44)
a 低血糖イベント0回と各グループのリスクより算出
b P<0.001,
2 test.
1980年から2002年
2003年から2007年
低血糖なし15,202名
1,572名が認知症 (10.34%)
低血糖あり1,465名
250名が認知症 (16.95%)
Whitmer, R. A. et al. JAMA 2009; 301: 1565-1572.
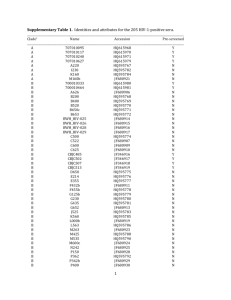
ADOPT
[海外データ]
治療薬別の空腹時血糖値の推移
(mg/dL)
160
4年時点におけるFPGの差(95%CI)
ロシグリタゾン vs メトホルミン
-9.8(-12.7~-7.0);p<0.001
グリベンクラミド
ロシグリタゾン vs グリベンクラミド
-17.4(-20.4~-14.5);p<0.001
150
メトホルミン
空 140
腹
時
血 130
糖
値
ロシグリタゾン
年間あたりのFPG増加量(95%CI)
ロシグリタゾン
0.7(0.2~1.1)
メトホルミン
2.7(2.3~3.2) *
グリベンクラミド 5.6(5.1~6.1) *
120
110
0
~
~
0
mean±SE
*:有意差あり vs ロシグリタゾン
1
2
追跡期間
3
4
5 (年)
症例数
4,118
3,408
3,054
2,647
2,242
840
2型糖尿病と診断され3年以内のドラッグナイーブ患者4,360例(30~75歳 空腹時血糖126~180mg/dL)を無作為に
チアゾリジン薬(ロシグリタゾン#)、ビグアナイド薬(メトホルミン)、SU薬(グリベンクラミド)に割り付け、盲験下で4~6年に
わたり単独投与を行い、血糖コントロールの推移を比較した。
#ロシグリタゾンは国内未承認
Kahn S. et al.:N.Engl.J.Med.,355,2427,2006.
SU薬とTZD薬の長期投与試験
HbA1cの推移
SU薬群のHbA1cの推移
TZD薬群のHbA1cの推移
▲
▲
■
●
◆
▼
■
●
◆
■
-1
◆
◆ ▼
▼
●
◆ ▼ ▲
▼ ▲
●
▲ ● ■
● ■ ●
■
●
◆
■
●
■
■ ■
▲●
▲
▲
■
■
■
▲
▲ ●
■
▲
◆
●
■
● ●
■
●
●
■
-2
0
▲
▼
■
◆
●
▼
◆
●
▲
▼
▼
●
■
◆
▲ ▲
●
▲ ▲ ▲ ▲
▲ ▲
▼
▼
▼ ▼
■ ■
■ ●
●
●
● ●
●
■ ■ ■ ■
-1
◆
●
▲
▼
▼
-2
0
◆
●
●
●
■
■
1
■
HbA1cの変化量
HbA1cの変化量
1
0
[海外データ]
1
2
3
4
観察期間
5
Alvarsson:SU薬 (n=39)
Alvarsson:SU薬 (n=48)
RECORD: SU薬 (n=272) / TZD (n=301)
Hanefeld: SU薬 (n=250) / TZD (n=250)
Charbonnel: SU薬 (n=313) / TZD (n=317)
UKPDS: (n=1,573)
6
◆
▲
▼
■
▼
10
(年)
0
1
2
3
観察期間
4
5
6
(年)
Chicago: SU薬 (n=230) / TZD (n=232)
ADOPT: SU薬 (n=1,441) / TZD (n=1,456)
PERISCOPE: SU薬 (n=181) / TZD (n=171)
Tan: SU薬 (n=297) / TZD (n=249)
Rosenstock:TZD薬 (n=115)
DeFronzo R.A. et al : Diabetes Care,58,773,2009.
糖尿病発症予防介入試験
event
per 1000
person-years
control
387
28.7
Placebo
Metformin
ILS
37
21
16
391
397
393
105.1
58.8
45.2
17
114
59.6
Placebo
37
122
121.3
Pioglitazone
11
86
42.6
-
3.0
Rosiglitazone
306
2365
43.1
Placebo
686
2634
86.8
2008
4.0
Pioglitazone
10
303
8.3
Placebo
45
299
37.6
2010
3.9
Met+Rosi
14
103
34.9
Placebo
41
104
101.1
publication
follow-up,
year
drug
*DPP
2005
0.9
Troglitazone
10
TRIPOD
2002
2.5
Troglitazone
PIPOD
2006
3.0
*DREAM
2006
*ACTNOW
*CANOE
Trial
No. of new
No.(total)
on-set of DM
No. of new
No.(total)
on-set of DM
event
per 1000
person-years
Thiazolidine
Other (α-GI, statin, fibrate, glinide)
WOSCOP
2001
5.0
Pravastation
57
2999
3.8
Placebo
82
3975
5.5
*STOP- NIDDM
2002
3.3
Acarbose
221
682
98.2
Placebo
285
686
125.9
BIP
2004
6.2
Bezafibrate
66
156
68.2
Placebo
80
147
87.8
*VICTORY
2009
4.0
Voglibose
50
897
13.9
Placebo
106
881
30.0
*NAVIGATOR
2010
6.5
Nateglinide
1674
3726
69.1
Placebo
1580
3747
64.9
*:エンドポイントとして設定あり
Matsuda M.;GEKKAN TOUNYOUBYOU;2,16-22,2010 2:16-22, 2010.
ピオグリタゾン
Bays H, Mandarino L, DeFronzo RA. J Clin Endocrinol Metab. 89:463-78, 2004. を日本人向けに描画
ピオグリタゾンの心血管イベント発症に対する影
対象:大血管障害の既往を有する2型糖尿病患者
響
大血管障害既往(5,238例)
評価項目
Hard endpoints
総死亡
Stroke既往
(984例)
心筋梗塞既往(2,445例)
MACE
MI
ACS
Stroke
●
心血管死
●
心筋梗塞
●
●
脳卒中
●
●
●
●
●
ACS
Hard
endpoints1)
リ
ス
ク
低
下
率
(%)
0
MACE2)
16%
0
10
NNT=48
20
p=0.027
MI3)
18%
0
28%
10
NNT=46
10
NNT=46
20
p=0.02
20
ACS3)
0
10
37%
0
NNT=44
10
20
20
30
30
30
30
30
40
40
40
40
50
50
50
50
p=0.045
Stroke4)
p=0.035
47%
NNT=21
40
50
p=0.009
1)Dormandy JA. et al.: Lancet, 366, 1279, 2005 2)Wilcox R. et al.: Am Heart J, 155:712, 2008
3)Erdmann. E. et al.:J.Am.Coll.Cardiol., 49,1772,2007 4) Wilcox R. et al.: Stroke, 38,865,2007.
[海外データ]
[海外データ]
ピオグリタオンはメトホルミンと比べ 総死亡のリスクが低い
総死亡のハザード比
0.5
1.0
2.0
*
1.40
第2世代SU剤
vsメトホルミン
*
0.92
ロシグリタゾン
vsメトホルミン
その他併用療法
vsメトホルミン
1.5
1.43
第1世代SU剤
vsメトホルミン
ピオグリタゾン
vsメトホルミン
(95%信頼区間)
**
0.62
***
1.01
***
**
*
p=0.0004
p=0.078
p<0.001
性別、年齢、糖尿病の罹病期間、心血管疾患の既往、心不全の既往、末梢動脈
疾患の既往、他の薬剤の有無、糖尿病合併症の既往で補正を行っている。
1990年-2005年の英国実地診療データベースより35歳から90歳の糖尿病患者91,521人を抽出し、
心筋梗塞、うっ血性心不全、総死亡の発生リスクを経口糖尿病薬別に比較検討した。
Tzoulaki et al.;BMJ,339,b4731,2009
Pioglitazone and bladder cancer risk:
a multipopulation pooled, cumulative exposure analysis
A
Association of cumulative
days of exposure (per 100
days) to pioglitazone with
bladder cancer incidence
within centres and
combined across centers
and combined across
centres in (a) men and (b)
women, with adjustment
for age, calendar year, and
ever exposure to
pioglitazone (logetransformed axis and
whiskers). (a) The absence
of ever exposure events in
Rotterdam prevented
convergence and hence is
excluded from the plot. (b)
The absence of ever
exposure events in
Manchester prevented
convergence and hence is
excluded from the plot.
B. Columbia, British
Columbia; Exp., exposed:
FE, fixed effects; RE,
random effects; Unexp.,
unexposed
Centre
Scotland
Finland
Events
Unexp. Exp.
543
23
Person-years
Unexp.
Exp.
711,917
38,586
RR [95% CI]
0.92 [0.83,1.02]
1,028
18
1,142,875
30,086
1.07 [0.98, 1.16]
B. Columbia
367
15
305,647
6,234
1.13 [1.01, 1.26]
CPRD
447
31
430,869
32,276
0.97 [0.91, 1.03]
Manchester
24
1
40,547
2,072
1.10 [0.87, 1.39]
FE: Q test p=0.03
1.01 [0.97, 1.05]
RE Model:
1.02 [0.94, 1.10]
0.75
1.00
1.25
1.50
Observed outcome
B
Centre
Scotland
Events
Unexp. Exp.
216
15
Person-years
Unexp.
Exp.
626,114
32,991
RR [95% CI]
1.03 [0.95, 1.12]
Finland
280
3
1,177,338
22,275
0.98 [0.75, 1.29]
B. Columbia
89
1
267,959
4,177
1.19 [0.78, 1.80]
CPRD
112
9
369,985
25,214
0.97 [0.85, 1.10]
Rotterdam
10
1
15,238
585
1.02 [0.69, 1.50]
FE: Q test p=0.88
1.01 [0.95, 1.08]
0.75
1.00
1.25
1.50
Observed outcome
Diabetologia DOI 10.1007/s00125-014-3456-9 posted online 3 December 2014
Multiple, Complex Pathophysiological
Abnormalities in T2DM
pancreatic
insulin
secretion
incretin
effect
_
gut
carbohydrate
delivery &
absorption
pancreatic
glucagon
secretion
?
HYPERGLYCEMIA
_
+
hepatic
glucose
production
renal
glucose
excretion
peripheral
glucose
uptake
Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011
Multiple, Complex Pathophysiological
Abnormalities in T2DM
GLP-1R
agonists
Insulin
Glinides S U s
incretin
effect
DPP-4
inhibitors
pancreatic
insulin
secretion
pancreatic
glucagon
secretion DA
Amylin
mimetics
_
agonists
AGIs
gut
carbohydrate
delivery &
absorption
?
HYPERGLYCEMIA
Metformin
Bile acid
sequestrants
SGLT2
inhibitors
_
+
hepatic
glucose
production
renal
glucose
excretion
TZDs
peripheral
glucose
uptake
Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011
Injectable
Class
Mechanism
Advantages
Disadvantages
Cost
Amylin
mime cs
• Ac vates amylin
receptor
• ¯ glucagon
• ¯ gastric emptying
• - sa ety
• ¯ Weight
• Gastrointes nal
• ¯ Postprandial glucose • Modest ¯ A1c
• Injectable
• Hypo if insulin dose
not reduced
• Dosing frequency
• Training requirements
GLP-1
receptor
agonists
• Ac vates GLP-1 R
• - Insulin, ¯ glucagon
• ¯ gastric emptying
• - sa ety
• ¯ Weight
• No hypoglycemia
• ¯ Postprandial glucose
• ¯ Some CV risk factors
• Gastrointes nal
High
• ? Pancrea s
• - Heart rate
• Medullary ca (rodents)
• Injectable
• Training requirements
Insulin
• Ac vates insulin
receptor
• Myriad
• Universally effec ve
• Unlimited efficacy
• ¯ Microvascular risk
• Hypoglycemia
• Weight gain
• ? Mitogenicity
• Injectable
• Pa ent reluctance
• Training requirements
Table 1. Proper es of an -hyperglycemic agents
High
Variable
Diabetes Care 2015;38:140-149;
Diabetologia 2015;10.1077/s00125-014-3460-0
Oral Class
Mechanism
a-Glucosidase • Inhibits a-glucosidase
inhibitors
• Slows carbohydrate
diges on / absorp on
Advantages
Disadvantages Cost
• No hypoglycemia
• Nonsystemic
• ¯ Postprandial glucose
• ? ¯ CVD events
• Gastrointes nal
• Dosing frequency
• Modest ¯ A1c
Mod.
DPP-4
inhibitors
• Inhibits DPP-4
• Increases incre n
(GLP-1, GIP) levels
• No hypoglycemia
• Well tolerated
• Angioedema /
ur caria
• ? Pancrea s
• ? - Heart failure
High
Bile acid
sequestrants
• Bind bile acids
• ? ¯ Hepa c glucose
produc on
• No hypoglycemia
• ¯ LDL-C
• Gastrointes nal
• Modest ¯ A1c
• Dosing frequency
High
Dopamine-2
agonists
• Ac vates DA receptor
• Alters hypothalamic
control of metabolism
• - insulin sensi vity
• No hypoglyemia
• ? ¯ CVD events
• Modest ¯ A1c
• Dizziness, fa gue
• Nausea
• Rhini s
High
SGLT2
inhibitors
• Inhibits SGLT2 in
proximal nephron
• Increases glucosuria
•¯ Weight
• No hypoglycemia
• ¯ BP
• Effec ve at all stages
• GU infec ons
High
• Polyuria
• Volume deple on
• - LDL-C
• -Cr (transient)
Table 1. Proper es of an -hyperglycemic agents
Diabetes Care 2015;38:140-149;
Diabetologia 2015;10.1077/s00125-014-3460-0
Oral Class
Biguanides
Mechanism
• Ac vates AMPkinase (?other)
• ¯ Hepa c glucose
produc on
Advantages
• Extensive experience
• No hypoglycemia
• Weight neutral
• ? ¯ CVD
Sulfonylureas • Closes KATP channels • Extensive experience
• - Insulin secre on
• ¯ Microvascular risk
Disadvantages
• Gastrointes nal
Low
• Lac c acidosis (rare)
• B-12
i defice ncy
• Contraindica ons
• Hypoglycemia
• - Weight
• Low durability
• ? Blunts ischemic
precondi oning
Megli nides
• Closes KATP channels • ¯ Postprandial glucose • Hypoglycemia
• - Insulin secre on
• Dosing flexibility
• - Weight
• ? Blunts ischemic
precondi oning
• Dosing frequency
TZDs
• PPAR-g ac vator
• - Insulin sensi vity
• No hypoglycemia
• Durability
• ¯ TGs (pio)
• - HDL-C
• ? ¯ CVD events (pio)
Table 1. Proper es of an -hyperglycemic agents
Cost
Low
Mod.
• - Weight
Low
• Edema/heart failure
• Bone fractures
• - LDL-C (rosi)
• ? - MI (rosi)
Diabetes Care 2015;38:140-149;
Diabetologia 2015;10.1077/s00125-014-3460-0
Healthy eating, weight control, increased physical activity & diabetes education
Monotherapy
Metformin
Efficacy*
Hypo risk
Weight
Side effects
Costs
Me ormin
intolerance or
contraindica on
Dual
therapy†
HbA1c
≥9%
Efficacy*
Hypo risk
Weight
Side effects
Costs
high
low risk
neutral/loss
GI / lactic acidosis
low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denote
any specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin
Metformin
Sulfonylurea
Thiazolidinedione
DPP-4
inhibitor
high
moderate risk
gain
hypoglycemia
low
high
low risk
gain
edema, HF, fxs
low
intermediate
low risk
neutral
rare
high
+
+
Metformin
Metformin
+
Metformin
+
+
Metformin
+
SGLT2
inhibitor
GLP-1 receptor
agonist
Insulin (basal)
intermediate
low risk
loss
GU, dehydration
high
high
low risk
loss
GI
high
highest
high risk
gain
hypoglycemia
variable
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denote
any specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin
+
Triple
therapy
Sulfonylurea
+
TZD
Uncontrolled
hyperglycemia
(catabolic features,
BG ≥300-350 mg/dl,
HbA1c ≥10-12%)
Metformin
+
Thiazolidinedione
+
Metformin
Metformin
+
+
DPP-4
Inhibitor
+
SU
SGLT-2
Inhibitor
+
SU
SU
Metformin
+
GLP-1 receptor
agonist
+
Metformin
+
Insulin (basal)
+
TZD
SU
or
DPP-4-i
or
DPP-4-i
or
TZD
or
TZD
or
TZD
or
DPP-4-i
or
SGLT2-i
or
SGLT2-i
or
SGLT2-i
or
DPP-4-i
or
Insulin§
or
SGLT2-i
or
Insulin§
or
Insulin§
or GLP-1-RA
or GLP-1-RA
or
or
Insulin§
or GLP-1-RA
Insulin§
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, add
basal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGL T2-i:
Metformin
Combination
injectable
therapy‡
+
Basal Insulin +
Mealtime Insulin or
GLP-1-RA
Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0
Pioglitazon と Alogliptinの併用効果
Screened
n=298
Failed screening
n=227
Placebo
n=24
Discontinued
n=0
Completed
n=24
n
Sex (% men)
Age (years)
Weight (kg)
BMI (kg/m2)
Systolic blood pressure (mmHg)
Diastolic blood pressure (mmHg)
Diabetes duration (years)
A1C (%)
Fasting glucose (mmol/L)
Anti-hyperglycemic agent (n, %)
Use of metformin (n, %)
Use of sulfonylurea(n, %)
Use of glinidines (n, %)
Randomized
n=71
Alogliptin 25mg
pioglitazone 30mg
n=22
Alogliptin 25mg
n=25
Discontinued
n=0
Completed
n=25
PBO
24
83
59.1±6.2
99 (93-111)
32.1±4.0
141±2
86±1
5.5±3.2
6.6±0.7
8.9±1.6
23 (96)
13 (57)
6 (26)
4 (17)
Discontinued
n=1
ALO
25
60
58.7±6.5
99 (85-102)
31.1±4.2
140±3
83±2
6.4±3.6
6.8±0.8
9.3±2.8
22 (88)
13 (60)
6 (28)
3 (12)
Completed
n=21
ALO/PIO
22
68
59.1±6.9
93 (86-103)
31.2±3.5
139±4
83±2
5.0±3.8
6.6±0.6
8.5±2.0
21 (95)
12 (57)
8 (38)
1 (5)
European Journal of Endocrinology 170: 565–574, 2014
Pioglitazon と Alogliptinの併用効果
0.4
0.0
-0.5
-0.4
-1.0
-1.5
C
14
12
10
8
6
4
Glucose (mmol/L)
***
Change in FPG
(mmol/L)
0.5
***
B
-0.9
PBO
ALO
●
■
▲
Week 0
1
0.7
**
***
**
0
-1
-2
-3
-1.2
-1.9
ALO ALO/PIO
ALO/PIO
D
PBO
PBO
14
● PBO
ALO
12
■ ALO
ALO/PIO
10
▲ ALO/PIO
8
6
4 Week 16
-1 0 1 2 3 4 5 6 7 8
Time (h)
-1 0 1 2 3 4 5 6 7 8
Time (h)
Change in AUC glucose
(mmol/L×8h)
1.0
***
Glucose (mmol/L)
Change in A1C (%)
A
***
E
10
6.7
**
***
0
-10
-20
-12.2
-22.1
-30
PBO
ALO ALO/PIO
Changes in parameters of glucose metabolism after treatment with alogliptin/pioglitazone
(ALO/PIO) combination therapy, ALO monotherapy, or placebo (PBO) treatment for 16 weeks.
A1C (A) and fasting glucose concentrations (B) were reduced by ALO/PIO combination
therapy to a greater extent than ALO monotherapy as compared with PBO. Similarly,
postprandial glucose levels were lower following ALO/PIO combination therapy then ALO
monotherapy as compared with PBO (C, D and E). **P<0.01; ***P<0.001.
European Journal of Endocrinology 170: 565–574, 2014
Pioglitazon と Alogliptinの併用効果
インスリン分泌の改善!
●
■
▲
750
1,000
PBO
ALO
ALO/PIO
Insulin secretion rates
(pmol/min per m2)
Insulin secretion rates
(pmol/min per m2)
1,000
500
250
0
8
11
■
▲
750
PBO
ALO
ALO/PIO
500
250
0
Week 0
5
●
14
Week 16
5
Glucose (mmol/L)
Weight (kg)
PBO
ALO
ALO/PIO
8
11
14
Glucose (mmol/L)
Week0
Week16
Change from
baseline
99 (93 to 111)
99 (85 to 102)
93 (86 to 103)
100 (94 to 112)
95 (84 to 102)
95 (89 to 101)
0.6 (-0.2 to 1.3)
-0.1 (-1.8 to 1.5)
1.4 (-0.2 to 2.5)
European Journal of Endocrinology 170: 565–574, 2014
Pioglitazone と SGLT-2阻害薬の併用
n
Age (years)
Men
Women
Race
White
African American
Asian
Other
HbA1c (%)
FPG (mg/dL)
FPG (mmol/L)
120-min PPG (mg/dL)
120-min PPG (mmol/L)
Weight (kg)
BMI
≥30kg/m2
≥25kg/m2
Duration of diabetes (years)
Data are means ± SD or n (%).
Placebo +
Dapagliflozin 5mg + Dapagliflozin 10mg +
pioglitazone ≥30mg pioglitazone ≥30mg pioglitazone ≥30mg
139
141
140
53.5 ± 11.4
53.2 ± 10.9
53.8 ± 10.4
71 (51.1)
78 (55.3)
59 (42.1)
68 (48.9)
63 (44.7)
81 (57.9)
102 (74.3)
6 (4.3)
24 (17.3)
7 (5.0)
8.34 ± 1.00
160.7 ± 47.0
8.92 ± 2.61
294 ± 81
16.3 ± 4.50
86.4 ± 21.3
102 (72.3)
9 (6.4)
26 (18.4)
4 (2.8)
8.40 ± 1.03
168.6 ± 52.1
9.36 ± 2.89
285 ± 99
15.8 ± 5.49
87.8 ± 20.7
101 (72.1)
7 (5.0)
21 (15.0)
11 (7.9)
8.37 ± 0.96
164.9 ± 46.3
9.15 ± 2.57
308 ± 93
17.1 ± 5.17
84.8 ± 22.2
85 (61.2)
122 (87.8)
5.07 ± 5.05
87 (61.7)
122 (86.5)
5.64 ± 5.36
72 (51.4)
130 (92.9)
5.75 ± 6.44
Diabetes Care 35: 1473–1478, 2012
Pioglitazone と Dapagliflozinの併用
HbA1c (%) Mean Change
from Baseline
0.0
-0.2
-0.4
-0.6
-0.8
-1.0
-1.2
-1.4
Week 48 Value (95% CI)
● 2.99 (2.19, 3.79)
■ 1.35 (0.61, 2.09)
▲ 0.69 (-0.03, 1.14)
4.0
Total Body Weight (kg) Mean
Change from Baseline
Week 48 Value (95% CI)
● -0.54 (-0.70, -0.38)
■ -0.95 (-1.10, -0.80)
▲ -1.21 (-1.36, -1.06)
0.2
3.0
2.0
1.0
0.0
-1.0
-2.0
0
8
16
24
32
Time (week)
Sample size per time point
Placebo 137 136 133 124 115 110 104
Dapa 5mg 139 137 131 133 132 126 122
Dapa 10mg 139 135 137 134 131 125 123
●
40
99
116
119
48
69
89
108
0
8
16
24
32
Time (week)
Sample size per time point
Placebo 139 125 138 136 134 124 115 108 105
Dapa 5mg 140 126 136 137 132 133 132 126 123
Dapa 10mg 140 128 138 136 137 134 131 125 124
40
100
117
119
48
69
89
108
▲ Dapagliflozin 10mg
Placebo (pioglitazone alone) ■ Dapagliflozin 5mg
Changes in glycemic parameters for placebo (circles), dapagliflozin 5 mg (squares), and dapagliflozin
10 mg (triangles) all plus pioglitazone ≥30 mg
LEFT: Mean change from baseline in HbA1c after adjustment for baseline value over time
RIGHT: Mean change from baseline in total body weight after adjustment for baseline value over time
Includes patients who took at least one dose of double-blind study medication
Error bars represent 95% CIs Treatment symbols shifted horizontally to prevent error bars from
overlapping
Diabetes Care 35: 1473–1478, 2012
Pioglitazone と Dapagliflozinの併用
Placebo +
Dapagliflozin 5mg +
pioglitazone ≥30mg pioglitazone ≥30mg
n
139
141
At least one adverse event
93 (66.9)
96 (68.1)
At least one serious adverse event
4 (2.9)
6 (4.3)
Adverse event leading to
discontinuation of study
5 (3.6)
5 (3.5)
medication
Most common adverse events (>5% in any treatment group)
Dyslipidemia
9 (6.5)
11 (7.8)
Nasopharyngitis
7 (5.0)
7 (5.0)
Diarrhea
6 (4.3)
5 (3.5)
Back pain
4 (2.9)
5 (3.5)
Upper respiratory tract infection
10 (7.2)
10 (7.1)
Headache
10 (7.2)
3 (2.1)
Pain in extremity
1 (0.7)
10 (7.1)
Edema peripheral
9 (6.5)
6 (4.3)
Adverse events of special interest
Suggestive of urinary tract
11 (7.9)
12 (8.5)
infection
Suggestive of genital infection
4 (2.9)
13 (9.2)
Mycotic genital infection
1 (0.7)
8 (5.7)
Decreased renal function
1 (0.7)
2 (1.4)
Fracture
0
2 (1.4)
Total patients with hypoglycemia
1 (0.7)
3 (2.1)
Major episode of hypoglycemia*
0
0
Congestive heart failure
1 (0.7)
0
Bladder cancer†
0
1(0.7)
Dapagliflozin 10mg +
pioglitazone ≥30mg
140
99 (70.7)
2 (1.4)
3 (2.1)
16 (11.4)
11 (7.9)
9 (6.4)
8 (5.7)
7 (5.0)
4 (2.9)
4 (2.9)
3 (2.1)
7 (5.0)
12 (8.6)
6 (4.3)
2 (1.4)
0
0
0
0
0
浮腫の
改善
UTIに
注意
Diabetes Care 35: 1473–1478, 2012
当院 pioglitazone 処方状況
actos
年度
2009
2010
2011
2012
2013
2013年度
actos
generic
liovelLD
liovelHD
合計
metformin
528
433
352
405
421
%
25.1
22.9
20.0
24.0
28.4
212
0
184
25
421
2014/10/1-2015/1/19
55.1
140
36.4
0.0
56
14.5
47.8
157
40.8
6.5
32
8.3
100
385
100
1535
1155
1210
882
752
%
73.1
61.0
68.9
52.2
50.6
経口血糖
降下薬
2100
1892
1757
1689
1485
埼玉医科大学総合医療センター 内分泌・糖尿病内科
2型糖尿病血糖管理
Durabilityの高い維持療法へのシフト
生活習慣介入: 栄養指導(管理栄養士),在宅療養指導(看護師)
各薬剤のMono therapy
インスリン強化療法
HbA1C≧10.0%
診断
HbA1C <7.0%
グリニド/DPP-4阻害薬
+
TZD/ビグアナイド薬
+
α-GI/SGLT-2阻害薬
HbA1C≧ 7.0%
SU/基礎インスリン
DPP-4阻害薬/GLP-1受容体作動薬
+
TZD/ビグアナイド薬
+
α-GI/SGLT-2阻害薬
川越市広報室撮影
2009年11月14日
ADA/EASDステートメントによる血糖降下薬の
特性
クラス
薬剤名
細胞メカニズム
ビグア
ナイド
メトホルミン
AMPキナーゼの
活性化
SU薬
第2世代
・グリブリド*/
グリベンクラミド
・グリピジド*
・グリクラジド
・グリメピリド
β細胞の
Kチャネルの閉鎖
・レパグリニド
・ナテグリニド
β細胞の
Kチャネルの閉鎖
グリニド
チアゾ
リジン薬
α-GI
DPP-4
阻害薬
・ピオグリタゾン
・ロシグリタゾン*
PPAR-γの活性化
作用機序
アドバンテージ
ディスアドバンテージ
コスト
肝臓での糖新生↓
・豊富な使用経験
・体重増加なし
・低血糖なし
・CVDイベント↓(UKPDS)
・消化器系副作用
・乳酸アシドーシス(まれに)
・ビタミンB12の欠乏
・多くの禁忌例(CKD、アシドーシスなど)
低
インスリン分泌↑
・豊富な使用経験
・最小血管障害リスク↓
(UKPDS)
・低血糖
・体重増加
・?プレコンディショニング低下
・Low Durability
低
インスリン分泌↑
・食後血糖上昇↓
・用量依存的
・低血糖
・体重増加
・?プレコンディショニング低下
・頻回服用
高
インスリン感受性↑
・低血糖なし
・Durability
・HDL-C↑
・TG↓
・CVDイベント↓(PROactive)
・体重増加
・浮腫/心不全
・骨折
・LDL-C↑(ロシグリタゾン)
・?心筋梗塞↑(メタアナリシス、
ロシグリタゾン)
・?膀胱癌↑(ピオグリタゾン)
高
・弱いHbA1c低下作用
・消化器系副作用
・頻回服用
中
・弱いHbA1c低下作用
・蕁麻疹/血管浮腫
・?膵炎
高
・アカルボース
・ミグリトール
・ボグリボース
α-グルコシダーゼ
の阻害
グルコースの
消化吸収遅延
・低血糖のなし
・食後血糖上昇↓
・CVDイベント↓(STOPNIDDM)
・局所作用
・シタグリプチン
・ビルダグリプチン
・サキサグリプチン
・リナグリプチン
・アログリプチン
DPP-4活性阻害、
食後のインクレチン
濃度の増加
・インスリン分泌↑
・グルカゴン分泌↓
・低血糖なし
・良好な忍容性
*国内未承認
(グルコース依存)
INZUCCHI S.E.;Diabetes Care,35,1364,2012.
ADA/EASD 血糖降下薬のアルゴリズム
健康的な食事、体重管理、身体活動の増加、糖尿病教育
単剤によ
る
治療開始
メトホルミン
単剤治療を3カ月間行ってもHbA1c目標値が達成できない場合、2剤併用療法へ(個々の患者および疾患特異的因子を考慮して選択)
2剤併用
治療
メトホルミン
+
+
+
+
+
スルホニル尿素薬
(SU薬)
チアゾリジン系
(TZD)
DPP-4阻害薬
(DPP-4-i)
SGLT2阻害薬
(SGLT2-i)
GLP-1受容体作動
薬(GLP-1-RA)
+
インスリン(基礎)
2剤併用治療を3カ月間行ってもHbA1c目標値が達成できない場合、3剤併用療法へ(個々の患者および疾患特異的因子を考慮して選択)
メトホルミン
3剤併用
治療
+
+
+
+
+
+
SU薬
TZD
DPP-4-i
SGLT2-i
GLP-1-RA
インスリン(基礎)
+下記1剤
+下記1剤
+下記1剤
TZD
DPP-4-I
SGLT2-I
GLP-1-RA
インスリン
+下記1剤
+下記1剤
SU薬
DPP-4-I
SGLT2-I
GLP-1-RA
インスリン
SU薬
TZD
SGLT2-I
インスリン
SU薬
TZD
DPP-4 I
インスリン
SU薬
TZD
インスリン
+下記1剤
TZD
DPP-4-I
SGLT2-I
GLP-1-RA
3剤併用治療を3カ月間行ってもHbA1c目標値が達成できず、3剤併用治療が①経口薬のみの組み合わせであった場合は注射製剤の組み
合わせに変更②GLP-1-RAを含む組み合わせであった場合は基礎インスリンを追加③至適用量の基礎インスリン治療を受けていた場合は
GLP-1-RAまたは食前インスリンを追加。治療抵抗性の場合にはTZDまたはSGLT-iの追加を考慮
注射剤の
併用
メトホルミン
+
基礎インスリン
+
食前インスリンまたはGLP-1-RA
出典:Diabetes Care 2015;38:S1-S94 改変