Andrea Vania
advertisement

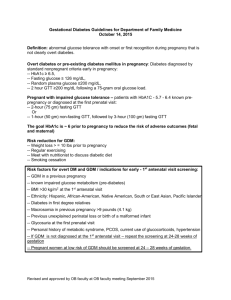
The risk of Insulin Resistence and Metabolic Syndrome among overweight/obese children born of mothers with Gestational Diabetes Mosca A., Vania A Dept. of Paediatrics and Paediatric Neuropsychiatry, “Sapienza” University of Rome, Italy Gestational Diabetes Mellitus • The incidence of Gestational Diabetes is increasing in the context of the pandemics in obesity and type 2 Diabetes Mellitus (1) • the Prevalence of GDM ranges from 2% to 6%, with much higher figures (up to 22%) in specific populations Asian (2) (1) Anna V et al.: Sociodemographic correlates of the increasing trend in prevalence of gestational diabetes mellitus in a large population of women between 1995 and 2005. Diabetes Care 2008;31:2288-93. (2) Galtier F.: Definition, epidemiology, risk factors. Diabetes Metab 2010;36:628-51. Definition of GDM GDM is defined as a carbohydrate intolerance, of variable severity, which is first recognized during pregnancy GDM encompasses 2 different entities: 1- glucose tolerance defect, that generally occurs in the second half of pregnancy and disappears (at least temporarily) after the delivery 2- prepregnancy diabetes (mainly DMT2 or NIDDM), only discovered during pregnancy, or triggered by pregnancy, that persists after delivery. Effect of Hyperglycemia on Fetal Growth In 2008, the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study (3): Relationship between high maternal plasma glucose and increased frequency of adverse perinatal outcomes Association between high maternal glycemia and fetal hyperinsulinism with birth weight >90th percentile Association of maternal glycemia values with excessive fetal growth, particularly of the fetus’ adipose tissue (3) (HAPO) Study - Diabetes 2009;58:453-9. Placental Modifications In GDM maternal metabolic environment is characterized by insulin resistance and inflammation: - The Insulin resistance facilitates maternal hypertriglyceridemia that enhances substrates availability to the fetus. Placental abnormalities are frequent in diabetic pregnancy:: - Genes for lipids transportation are upregulated in the placenta, as well as genes for inflammation - The epigenetic adaptations to a detrimental in-utero environment may affect the short- and long-term metabolic regulation of the newborn Maternal Diabetes during pregnancy is a risk factor for MACROSOMIA Neonatal Complications Neonatal Respiratory Distress The risk of birth injury was the highest for infants with a birth weight of 4500-4999 g and >5000 g (OR 2.4 [95% CI 2.2-2.5] and 3.5 [3.0-4.2]) (4) Correlation between increased cord Cpeptide levels, macrosomia, and hypoglycemia (5) Fetal and Neonatal Malformations The risk for congenital malformations in preexisting diabetes is 1.9- to 10-fold higher than that in the total population. (6) (4)Esakoff TF et al.: The association between birthweight 4000 g or greater and perinatal outcomes in patients with and without gestational diabetes mellitus. Am J Obstet Gynecol 2009;200:672.e1-e4. (5) Sosenko IR et al.: The infant of the diabetic mother: correlation of increased cord C-peptide levels with macrosomia and hypoglycemia. N Engl J Med 1979;301: 859-62. (6) Allen VM et al.: Teratogenicity associated with pre-existing and gestational diabetes. J Obstet Gynaecol Can 2007;29:927-34. Our study… An increased risk of developing MS after 10 years of life in children born to mothers with DG and showing higher values of WC and BMI at the time has been found (7). Insulin Resistance Metabolic Syndrome mothers with GDM (7) Nehring I et al.: Gestational diabetes predicts the risk of childhood overweight and abdominal circumference independent of maternal obesity. Diabet Med 2013 2380 Overweight or Obese Children 2042 children born to mothers NoGDM Male Female 338 children born to mother GDM 44,03 14,2 55,97 85,8 GDM NoGDM Anthropometric and laboratory parameters Our study… METABOLIC SYNDROMECRITERIA WC ≥ 95°th PAS-PAD ≥ 95°th Tg ≥ 95°th HDL ≤ 5°c Gli ≥ 100mg/dl HOMA-IR ≥ 2.5 * * NoGDM GDM *Mann-Whitney -test p<0.05 Odd Ratio Insulin Resistence vs. GDM 95% CI, 8.44 -16.57, p=0.0001 Metabolic Syndrome vs. GDM 95% CI, 1.29 -2.39, p=0.003 Conclusions (1) In our population, overweight/obese children born to mothers with GDM tend to have a greater prevalence of “central” obesity than children born to mothers non-GDM. All of them have a very high risk of developing Insulin Resistance, and a greater likelihood to develop a Metabolic Syndrome. Conclusions (2) The specific mechanisms of the long-term effects of GDM on the child remain unclear. But the link between epigenetic placental changes and foetal ones, leading to Childhood Diabetes and Obesity, is more and more clear. There is an association between an altered intrauterine environment and some epigenetic changes in the newborn. Intrauterine exposure to hyperglycaemia has a negative impact on long-term outcomes, although it is difficult to separate these from the effects of maternal obesity. Preventing GDM can be a valid way to prevent a certain number of cases of Childhood Obesity or – at least – to limit their progression to more severe expressions of it, such as super-obesity, insulin resistance, and NIDDM.