Forearm,Montegia&Galleazzi Fractures Dislocations
advertisement

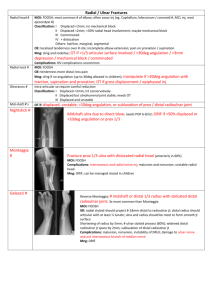
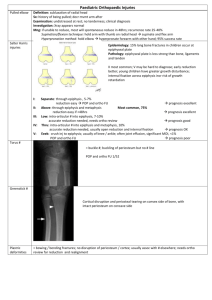
دکتر اکبری اقدم استادیار دانشکده پزشکی اصفهان Common 12 to 16y Most common site for refracture Fx suspected >>child has not returned all normal arm function within 1 to 2 days of injury Practical classification 2 bones 3 levels 4fracture patterns (Bow,Greenstick,Compelet&Comminuted) Closed Reduction still remains the gold standard for closed isolated pediatric forearm fractures Non or minimally displace Long arm cast(except above 4 y with stable distal third fx) 1 and 2 week visit 6-8 week cast After that splint until union compelet Displaced fractures Manipolation with sedation Contorol with fluroscopy Sugar tong splint(7-10 layers 3inch plaster) Next week x-ray and change splint to cast 2 next weeks follow up 4 weeks after reduction can chang short cast Except under 4 y Return to sport now if… Distal third< 20 degree Middle third< 15 degree Upper third <10 degree 100% translation with <1cm shortening Rotation< 45 degree.difficult to measure Bicipital tuberisity and radial styloid Open fracture Fracture with unacceptibale reduction Fx in assosiated supracodylar fx(to avoid risk of compartement syn) Interamedullary fixation is preferred If one bone fixation Fix ulna If both bone should be fix,radius first 2-2.5 mm nail brace or cast 6-12 mo nail removal Redisplacement Forearm stiffness Refracture Malunion Nonunion Cross union(synostosis) Infection … Type 1 Ant dis radial head associated with ulnar diaphyseal fx at any level(most common) Ant radial head dislocasion (include pulled elbow) No plastic deformity of ulna Ant dis radial head with radial neck fx Ant dis radial head with fx of radial diaphyseal fx proximal to ulnar fx …. direct blow theory Hyperpronation theory Hyperextention theory Fusiform swelling elbow Pain &limit ROM elbow Three steps: Correcting the ulnar deformity Stable reduction of radial head Maintaining ulnar length and fx stability A bivalved long arm cast 4-6 w slight supination and elbow 90 to 110 flex Radiography every 1 to 2 w Hardware remove Congenital Posterior Bilateral Can be associated with various syndromes Traumatic Isolated ant. Or ant lateral dislocation Unless congenital or systemic difference Posterior monteggia fx dx Rare in children usully older patient Mechanism Direct force,sudden rotation and supination Suddenly loaded in longitodinal direction elbow at 60 flex Incomplete fx ulna>>close reduction casting in extension If doubt>>interamedullary fixation Comminuted or very proximal ulnar fx>>open reduction plate screw Lat swelling,varus,significant limitation of ROM Mechanism>>hyperextesion of elbow combined with pronation Incomplete or plastic deformation of ulna Close reduction >> Elbow in extension longitudinal traction valgus sterss test Long arm cast elbow 70 to 80 flex Ant dis with fx both radius and ulna Radial fx level same or distal too ulnar fx Fx unstable fixation Chronic Monteggia Injury Under 12 years old MRI Determine congruency radial head and capitellum Surgery Radial nerve identify Anconeous-extansor carpiulnaris interval Repair or reconsteraction of annular lig Radius head unreduceable >>ulnar osteotomy After radial head redauction>>anullar lig repi Fracture of the distal radius with DRUJ disruption Mechanism >>axial load ,forearm rotation Signs &symptoms>>pain,limitation of forearm rotation,wrist flex ext Type 1 dorsal (apex volar)displacment Type 2 volar(apex dorsal)displacment Galeazzi equivalent Distal radius fx with distal ulnar physis disruption Volar apex Radius fx greenstick or incomplete Close reduction and long arm cast in supination Complete fx Open reduction and fix with plate Incompelet radius fx Close reduction Compelet fx Open reduction