GEOG220 Lecture27 - The war on ebola
advertisement

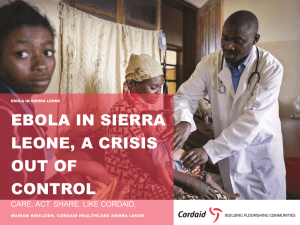
Thelma Kaime prepares to enter an isolation ward for Ebola patients in Monrovia. Her safety gear includes: rubber gloves, a Tyvex suit, rubber boots, a face mask, goggles, a hair net, a hood and an apron. Glenna Gordon for The Wall Street Journal Poverty and the ‘War on Ebola’ GEOG 220 - Geopolitics This class • Perspectives on the ‘Ebola crisis’ • Sustainable and socially just responses to epidemics Thinking about epidemics spatially and temporally “Epidemics implicate a diversity of spatial scales – from the individual diseased body to the globe – as well as temporal ones, as short-term outbreaks interact with longer term predisposing conditions, stresses and drivers.” Leach et al., 2010 Disaster analysis Thinking about responses critically “… particular framings of ‘the problem’ and governance processes and architectures have become mutually supporting and interlocked. Yet we also expose their serious shortcomings with respect both to their ability to deal with the full range of dynamics involved, and their implications for equity and social justice” Leach et al., 2010 Multiple framings of a social–ecological–technological system (adapted from Stirling, 2007 – Leach et al, 2010). • Complex systems perspective • Normative emphasis on reductions in poverty and social injustice socio-technological–ecological response system not only aiming at sustainable solutions, but also solutions that are experienced as appropriate and just by local populations • “Dominant narratives around Ebola … emphasise short-term, acute outbreaks requiring rapid identification and control—to ‘stamp out’ the outbreak and prevent dangerous spread to neighbouring and ultimately global populations” locked downs and closed borders • “Alternative narratives and models of “local intervention … focusing on active intervention in a particular setting to reduce disease risk and exposure” => Monitoring and addressing disease ecology and socio-natural relations and co-evolution • “Local knowledge, practices and concerns can inform and be integrated into participatory surveillance and response strategies, helping to make these more context-specific, locally appropriate and acceptable” Rethinking the basis of health Pre-conditions to health: • Peace • Shelter • Food • Income • Status of women, availability of health workers, costs/price of medicine Rethinking disease geopolitics • Dominant versus marginalized narratives • Power relations and politics • Politics of space – Control of the spatial representations and dimensions of diseases Ebola Hemorrhagic Fever • 1976: first recorded human cases near the Ebola river, in Zaire (now Democratic Republic of the Congo), and border regions with Sudan (now South Sudan), and Central African Republic Ebola Virus Prototype Viral Hemorrhagic Fever Pathogen Filovirus: enveloped, non-segmented, negativestranded RNA virus Severe disease with high case fatality >20 previous Ebola and Marburg virus outbreaks 2014 West Africa Ebola outbreak caused by Zaire ebolavirus species (five known Ebola virus species) Absence of specific treatment or vaccine From CDC Ebola Virus Zoonotic virus – bats the most likely reservoir, although species unknown Spillover event from infected wild animals (e.g., fruit bats, monkey, duiker) to humans, followed by human-human transmission From CDC Why is it such a concern? • c.50% death rate • Transmission through bodily fluids, though not aerosols (‘airborne’) • Initial denial and resistance to allow access to the sick and dead • Limited capacity to isolate patients and treat them Sub-regional diffusion • Guinea Sierra Leone Liberia • Nigeria Senegal 2014 Ebola Outbreak, West Africa WHO Ebola Response Team. N Engl J Med 2014. DOI: 10.1056/NEJMoa1411100 http://www.nejm.org/doi/full/10.1056/NEJMoa1411100?query=featured_ebola#t=articleResults From CDC International diffusion Explanatory factors • Prevailing poverty – Predatory, repressive or neglectful colonial and postindependence regimes => distrust of the government – Civil wars in Liberia and Sierra Leone => High poverty levels (G: 47%; L: 65%; SL: 50%) => Poor access to sanitation => Health services further weakened • Mistrust of state institutions, incl. health services “The people could just go hide in the bush” to avoid health workers, said Pascal Piguet, a Doctors Without Borders official in the adjoining district, Guéckédou [Guinea], where the outbreak was first identified in March. “They thought we were the vectors.” http://www.nytimes.com/2014/11/17/world/africa/fear-of-ebola-opens-waryvillages-to-outsiders-in-guinea.html Spatiality of transmission • • • • Home of infected people Burial sites Hospitals Markets and transport hubs • Regional-level interactions – ECOWAS – Migrant labor – Border markets Gendered vulnerability • Caring a mostly gendered activity – Care for sick people or deceased – Daily reproductive labor, incl. contacts at market places => 60-70% of Ebola deaths are women & girls International responses • Geopolitics of responses who did what, where? • Canada: – no medical staff send (Canada: 1 doctor/470 people in Canada compared to 1/33,000 in SL) – Visa to Canada suspended for people from affected countries (unlike US who feared ‘back-door’ entrance and end to air traffic providing supplies and staff) • Medecins Sans Frontiere/Doctors Without Borders: key role Domestic responses • Awareness campaign • Collection, isolation and treatment of patients • State of emergency (August – lifted 13 Nov in L) – Lock-downs: schools and universities closed; – Arrest of at least one journalist making “disparaging and inflammatory statements”, according to the Gvt of SL State of emergency in Sierra Leone One of the great, under-recognized successes of the response to HIV and AIDS in Africa was that the spread of an incurable sexually transmitted infection did not lead to repressive measures or massive stigmatization. On the contrary, the United Nations and donors insisted that public health be linked to human rights, and civil society organizations and people living with HIV and AIDS be represented in the governance of UNAIDS and the Global Fund. That is the polar opposite of the war-like approach to Ebola. The Sierra Leonean journalist Oswald Hanciles drew out the implications of Koroma’s “war” on Ebola, comparing it favorably with the weak government defenses against the rebel attacks fifteen years ago: “This strategy of energizing and mobilizing youth to ‘comb’ their neighborhoods to ferret out ‘Ebola suspects’ could be the most potent in this Ebola War. We are optimistic that the President would use the security forces to back up the youths who the President said should be ‘hard.’” That would be a frightening prospect. Vigilante mobs dragging people from their homes or sealing off neighborhoods would destroy the public trust and community involvement at the heart of good public health practice. State of Emergency in Liberia “The essence of the state of emergency was to curtail rights of her opponents,” said [opposition MP, Mr. Gray]. “Initially I did not support the state of emergency because it was not clearly defined. The significance of the state of emergency has not been seen.” http://www.nytimes.com/2014/11/14/world/africa/president-ellen-johnson-sirleaf-ends-stateofemergency.html?action=click&contentCollection=Africa&region=Footer&module=MoreInSec tion&pgtype=article Critiques of under-budgeted health care systems – Sierra Leone and Spain • Against ‘sick states’… Ebola protests in Spain • http://somatosphere.net/2014/10/againstsick-states.html Biopolitics of confinement • Securitization: seeing and engaging with an issue through the lens of ‘security’ => enables the use of extraordinary means (and a move away from usual political processes) in the name of security • Militarization: seeing and engaging with an issue through the military and banalization of military force Securitization of Ebola outbreak • Seeing affected countries, but also Africa and Africans through the fear of Ebola • Precautionary measures taken – People coming from Africa – Formerly infected persons (who are now immune) Ebola virus in Kono district • Kono district: main diamantiferous area in Sierra Leone • First confirmed case on 29 July 2014 • Under lock down