Procedures
advertisement

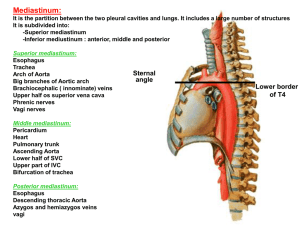
OVERVIEW OF ORGAN RECOVERY Elizabeth A. Davies, MD January 18, 2010 Procurement of the Heart Mobilizing the Heart • Open the Chest & open the pericardium • Assess the donor heart • Evaluate the contractility and coronary anatomy • Surgeon procuring the heart makes final decision • Chest is not open on the recipient at this point • If the donor heart unsuitable for transplant, the procedure can still be abandoned at this point. Mobilization of the Heart Base and diaphragmatic surface of heart Mobilizing the Great Vessels The vessels are mobilized widely to allow the organs to be removed expeditiously. • (4) The superior vena cava is dissected free. • (6) The innominate artery is completely mobilized • (7) The aortic arch is encircled just below the great vessels of the head and neck. • Dissection is carried along the aorta to its root. • (8,9) The left and right pulmonary arteries are mobilized. 6 Mobilization of the Great Veins Mobilization of the Great Arteries Procurement of the Lungs Pulmonary Assessment • Pleural spaces are opened and the lungs inspected. • The left and right pulmonary arteries are mobilized. • The trachea is isolated from the esophagus and encircled. Pulmonary Vessels, seen in a dorsal view of the heart & lungs. Cannula Placement • (10) A cardioplegia catheter is inserted into the proximal ascending aorta and held in by a pursestring suture. • A pulmoplegia catheter is inserted into the proximal pulmonary artery and held in by a pursestring suture. Mobilization of the Great Arteries Procurement of Abdominal Organs Dissection of the Retroperitoneum • The right colon and distal ileum are mobilized along the avascular planes exposing the Inferior Vena Cava and Aorta • A Kocher maneuver is performed by dividing the retroperitoneal attachments along the lateral border of the second and third portion of the duodenum. • (30) The duodenum is swept medially to provide access to the left renal vein, infrahepatic vena cava and SMA. • The left renal vein is identified crossing the aorta. Mobilization of the Right Colon The Duodenum and Pancreas Exposure of the Right Retroperitoneum • The inferior mesenteric artery is identified and divided exposing the left side of the aorta. • The distal aorta is mobilized just proximal to its bifurcations. • Care must be taken to not injure renal arteries potentially arising from the common iliac arteries The Retroperitoneum and Great Vessels Mobilization of the Liver • Take down the diaphragmatic attachments of the left lobe of the liver. • Identify the presence/absence of an accessory left hepatic artery (branch of left gastric artery) in gastrohepatic ligament • Divide the gastric and esophageal branches of the left gastric artery. Mobilization of the Liver; Identifying the hepatic artery Isolation of the Supraceliac Aorta • (17) Mobilize the Aorta where it passes through the crura of the diaphragm. • This enables the surgeon to place clamps superior to the celiac axis to perfuse the liver and kidneys without perfusing the heart. Isolation of Supraceliac Aorta Procurement of the Pancreas Exposing the Pancreas • The omentum is taken off the transverse colon in an avascular plane opening the lesser sac and allowing visualization of the pancreas body and tail. • (4) This dissection is facilitated by upward traction of the stomach and inferior retraction of the transverse colon. Dissection of the Inferior Border of the Pancreas Mobilizing the Descending Colon and the Left Kidney • The left colon is mobilized along an avascular plane between the colon and the left kidney. • The spleen is mobilized along its diaphragmatic plane • The inferior border of the pancreas is divided allowing the spleen and pancreas to be mobilized medially Mobilization of the Distal Pancreas Dividing the Stomach • The short gastric arteries between the stomach and spleen are ligated and divided. • The stomach is infused with 100-200 cc of betadine. • A GIA stapler is used to divide the duodenum just distal to the pylorus. – The stomach is retracted toward the left chest Division of the Duodenum Procurement of the Liver Dissection of the Porta Hepatis • Identify and divide the common bile duct • (11) Identify the hepatic artery and trace back towards the celiac axis. • (12,13) The gastroduodenal artery (branch of the hepatic artery) is isolated. • The splenic and left gastric arteries are then identified. Division of Common Duct and Drainage of the Gallbladder Normal Variants of Hepatic Arterial Anatomy • Left Accessory Hepatic Artery: 23% donors – branch from the left gastric artery and supplies the left lobe of the liver. • Replaced Right Hepatic Artery: 12 % donors branches from the superior mesenteric artery, passes behind the common duct to the right lobe. Division of Common Duct and Drainage of the Gallbladder Dissection of the Porta Hepatis • A longitudinal incision is made in the inferior surface of the fundus of the gallbladder. • (32) The biliary tree is flushed with saline through the gallbladder. • This flushes bile before endothelium is exposed – bile is toxic to endothelial cells Procurement of the Kidneys Procurement of the Kidneys • Isolate the ureters as they cross the common iliac artery bifurcation • If cannulating the inferior vena cava (lung recovery), insure that no low-lying right renal artery crosses anterior to the IVC The Retroperitoneum and Great Vessels Cannulating the Aorta, Vena Cava & Portal Vein • (45) An inflow catheter is placed in the aorta • (48) A cannula is passed into the portal vein through a transverse venotomy made in the inferior mesenteric vein. Pancreatic Anatomy Cannulation of the Aorta and the Vena Cava Preparing for Cross-Clamp • Heparin is given. • Cold lactated ringers should begin flushing through the portal vein catheter. • 1 - 2 liters of cold fluid should run through the portal catheter every 20 minutes for adults (500 ml in children). Cross-Clamp • After heparin has circulated for three minutes, (52) the aorta is cannulated. • For lung procurement, PGE1 is infused just prior to cross-clamp. • The aorta is occluded at the level of the diaphragm by a vascular clamp. • Simultaneously, the perfusion solution (LR, UW, HTK, etc.) is infused into the heart, liver, kidneys, and pancreas via inflow catheters. Mobilization of the Suprahepatic Vena Cava • At crossclamp, the thoracic and abdominal surgeons agree on the point of division of the suprahepatic inferior vena cava. – Incidence of pacemaker dependency reportedly less in cava to cava anastomosis in heart transplant – Need suprahepatic cava to perform anastomosis in liver transplant • A rim of the diaphragm is left attached to the suprahepatic vena cava (37) Mobilization of the Suprahepatic Vena Cava Excision of the Donor Heart • (55) Superior vena cava is ligated and divided. • (57) The aorta is cross-clamped at the aortic arch and (58) divided just proximal to the cross-clamp. • (54) Cardioplegia is completely infused (59,60) • The pulmonary artery (main branches) are divided, (61) the heart is elevated (next slide) and the pulmonary veins (62) are divided. Excision of the Donor Heart Division of the Pulmonary Veins Excision of the Lungs • Pulmonoplegia is completely infused. • The pulmonary veins are divided with consensus between heart and lung team • The pulmonary artery main branches are divided. • The lungs continue to be fully ventilated. • With full inspiration, the trachea is stapled and divided. • The lungs are removed from the pleural cavities. Division of the Small Bowel Mesentery • While the chest surgeons recover the thoracic organs, the distal duodeum is divided. • The small bowel mesentery is divided away from the pancreas at the base of the mesentery. • The arterial and venous branches are ligated on the pancreatic side. Isolation of the Infrahepatic Vena Cava • The inferior vena cava superior to the level of the renal veins is mobilized. • The liver is retracted upward and the right adrenal gland is divided with the adrenal vein going with the liver. • The right and left renal veins are identified and the inferior vena cava divided above them. The Retroperitoneum and Great Vessels Removal of En bloc Liver-Pancreas • Ligate the SMA at its origin • Divide the SMA labeling the pancreas side with a vascular suture • Place a clamp above the SMA • Divide the aorta just above the clamp to continue perfusion to the kidneys. • Divide the supraceliac aorta just distal to the cross clamp • The posterior and adventitial attachments of the vena cava and aorta are divided and the organs removed. Splitting the Pancreas and the Liver • Divide the splenic artery just distal to its origin from the celiac axis. • The gastroduodenal artery is ligated on the pancreatic side and divided. • The portal vein is divided at the superior border of the pancreas. • Adventitial attachments are divided, thus, splitting the liver and the pancreas. Posterior Aspect of the Entire Gland Backtable Perfusion of the Pancreas and Liver • The portal vein is perfused with UW • The hepatic artery, splenic artery and SMA are each perfused UW • Amphotericin B (50mg) is injected into the distal duodenal segment. Preparing the kidneys for removal • The vena cava and the aorta have been divided above the renal veins and arteries. • They are now divided below the cannulas’ insertion points. • The ureters are divided near the bladder. • The kidneys are mobilized outside Gerota’s fascia and removed from the abdomen en bloc. Preparing the Kidneys for Removal Backtable preparation of kidneys • The kidneys are placed posterior side up. • The proximal end of the aorta is oversewn and the clamp removed. • The lumbar arteries are clipped at their origin from the aorta. • The arterial anatomy of the kidneys is identified. • Gerota’s fascia is removed from the kidneys. – Care must be taken not to strip perihilar fat from the pelvis of the kidneys and to preserve all vascular branches to the ureters. Backtable preparation of kidneys • The kidneys are placed anterior side up. • The left renal vein is divided off the cava at its insertion. • The arterial anatomy of the kidneys is confirmed. • The kidneys are placed en bloc on pulsatile preservation. • For cold stored kidneys, the aorta is divide down the middle and the kidneys split. Splitting the Kidneys Facts about Cannulation Techniques • Perfusing enbloc preserves maximum renal arterial length and prevents intimal damage to the renal arteries. • Cannulating an aortic conduit is the ideal technique for the perfusion of a kidney with multiple renal arteries because it permits the use of one or more Carrel patches for renal arterial anastomosis. Pillings (Bulldog) Cannulation Technique Straight Cannulation Technique