counter current multiplication and micturation

Counter Current Multiplication.
And Micturition Reflex
Dr.Mohammed Sharique Ahmed Quadri
Assistant professor physiology
Al Amaarefa College
Objectives
• Describe the factors that determine the ability of loop of Henle to creat osmotic medullary gradient
• Identify countercurrent multiplier and countercurrent exchange systems in concentrating and diluting urine
• Explain changes in osmolarity of tubular fluid in the various segments of the loop of Henle when concentrated urine is being produced.
• Describe the role of ADH on the ability of the kidney to produce either a dilute or a concentrated urine.
• Discuss the micturition reflex.
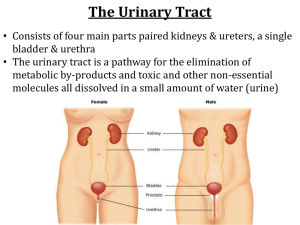
Urine Excretion
• Depending on the body ’ s state of hydration, the kidneys secrete urine of varying concentrations.
• Too much water in the ECF establishes a hypotonic ECF.
• A water deficit establishes a hypertonic ECF.
• This function is determined by the amount of water reabsorption in the renal tubules.
Urine Concentration & Dilution
• Water reabsorption is obligatory in the proximal(65%) tublues and Loop of Henle(15%).
• The final adjustment of the urine volume and osmolarity depends on the extent of facultative water reabsorption in the Collecting Ducts, which is depends on:-
– The blood level of antidiuretic hormone (ADH).
– The Medullary interstitium (MI) hypertonicity
(Medullary concentration gradient).
Urine Concentration
Requirements for forming a concentrated urine are:
High level of ADH (increase permeability)
High osmolarity of the renal medullary interstitial fluid (osmotic gradients)
Driving force for H2O reabsorption
• Driving force for water reabsorption throughout the entire length of tubules is an osmotic gradient between tubular lumen and surrounding interstitial fluid.
Urine Excretion
• A large, vertical osmotic gradient is established in the interstitial fluid of the medulla
(from 100 to 1200 mosm/liter)
• This osmotic gradient exists between the tubular lumen and the surrounding interstitial fluid.
Urine Concentration & Dilution
What is the process by which renal medullary interstitial fluid becomes hyperosmotic?
This process involves the operation of the medullary countercurrent system
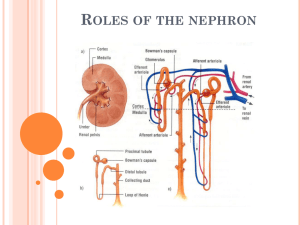
Medullary Countercurrent system
• Juxta medullary nephrons
– long loop of henle estabilishes a vertical osmotic gradient (Countercurrent multiplier) ,
– their vassa recta preserve this gradient while providing blood to renal medulla ,( Countercurrent exchanger)
– collecting ducts of all nephrones use the gradient in conjunction with the hormone vassopressin, to produce urine of varying concentration ( osmotic equilibrating device) .
• Collectively this entire functional organization is known as medullary countercurrent system
Countercurrent Multiplication
• Comparing the descending and ascending limbs of the loop of Henle
• The descending ling is highly permeable to water but does not extrude sodium for reabsorption.
• The ascending limb actively transports NaCl out of the tubular lumen into the surrounding interstitial fluid.
It is impermeable to water .
Therefore, water does not follow the salt by osmosis.
• There is a countercurrent flow produced by the close proximity of the two limbs.
Countercurrent Multiplication
Countercurrent Multiplication
Countercurrent Multiplication
Countercurrent Multiplication
Countercurrent Multiplication
Countercurrent Multiplication
Countercurrent Multiplication
BENEFITS OF COUNTERCURRENT
MULTIPLICATION
1. It establishes a vertical osmotic gradient in the medullary interstitial fluid. This gradient, in turn, is used by the collecting ducts to concentrate the tubular fluid so that a urine more concentrated than normal body fluids can be excreted.
2. Second, the fact that the fluid is hypotonic as it enters the distal parts of the tubule enables the kidneys to excrete a urine more dilute than normal body fluids.
Role of Vasopressin
•
Vasopressin-controlled, variable water reabsorption occurs in the final tubular segments.
• 65 percent of water reabsorption is obligatory in the proximal tubule. In the distal tubule and collecting duct it is variable, based on the secretion of ADH.
•
The secretion of vasopressin increases the permeability of the tubule cells to water. An osmotic gradient exists outside the tubules for the transport of water by osmosis.
• Vasopressin works on tubule cells through a cyclic AMP mechanism.
• During a water deficit, the secretion of vasopressin increases.
This increases water reabsorption.
• During an excess of water, the secretion of vasopressin decreases. Less water is reabsorbed. More is eliminated.
Mechanism of action of Vasopressin
Regulation of H
2
O reabsorption in response to H
2
O deficit
Regulation of H
2
O reabsorption in response to H
2
O Excess
Countercurrent exchange within the vasa recta conserves the medullary vertical osmotic gradient .
Renal Failure
• Causes of renal failure
– Infectious organisms
– Toxic agents
– Inappropriate immune responses
– Obstruction of urine flow
– An insufficient renal blood supply
Micturition
• Urine stored in bladder is eliminated by micturition
• Urine in bladder stimulates stretch receptors
• Stimulated stretch receptors signal smooth muscle in bladder wall by parasympathetic neurons
• Contraction of bladder pushes urine out of the body
• Micturition reflex
– Relaxation of external urethral sphincter muscle allowing urine to pass through urethra and out of the body
• Under voluntary control but cannot be delayed indefinitely
• Urinary incontinence
– Inability to prevent discharge of urine
Reflex and Voluntary Control of Mictrurition
Abnormalities of micturition
Atonic Bladder Caused by Destruction of Sensory Nerve
Fibers.
• Micturition reflex cannot occur if the sensory nerve fibers from the bladder to the spinal cord are destroyed.
• Person loses bladder control
• Instead of emptying periodically, the bladder fills to capacity and overflows a few drops at a time through the urethra. This is called overflow incontinence.
• A common cause of atonic bladder is crush injury to the sacral region of the spinal cord.
• Certain diseases can also
• Automatic Bladder Caused by Spinal Cord Damage
Above the Sacral Region.
• Typical micturition reflexes can still occur.
• They are no longer controlled by the brain.
• During the first few days to weeks the micturition reflexes are suppressed because “spinal shock” (sudden loss of facilitative impulses from the brain stem and cerebrum).
• Gradually typical micturition reflexes return; then, periodic (but unannounced) bladder emptying occurs.
• Some patients can still control urination in this condition by stimulating the skin (scratching or tickling) in the genital region, which sometimes elicits a micturition reflex.
• Uninhibited Neurogenic Bladder Caused by Lack of Inhibitory Signals from the Brain.
• Which results in frequent and relatively uncontrolled micturition.
• From partial damage in the spinal cord or the brain stem that interrupts most of the inhibitory signals.
• Facilitative impulses passing continually down the cord -even a small quantity of urine elicits an uncontrollable micturition reflex, thereby promoting frequent urination.
References
• Human physiology by Lauralee Sherwood, seventh edition
• Text book physiology by Guyton &Hall,11 th edition
• Text book of physiology by Linda .s contanzo,third edition


![Countercurrent exchange in biological systems [edit]](http://s3.studylib.net/store/data/006922309_1-6a35e93b26f21c65b0a52d93cac8962b-300x300.png)