Skin and Body Senses
advertisement

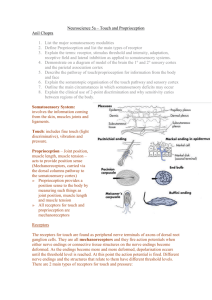
SKIN AND BODY SENSES OVERVIEW OF QUESTIONS • Are there specialized receptors in the skin for sensing different tactile qualities? • What is the most sensitive part of the body? • Is it possible to reduce pain with your thoughts? TOUCH THERAPY OF NEWBORNS • Touch Research Institute • Established in 1992 by Director Tiffany Field, Ph.D. at the University of Miami School of Medicine. • Premature infants got little tactile stimulation. • Trained senior citizens to give massages. • Many benefits to babies and seniors. BENEFITS OF MASSAGE • • • • • • • • • • Compared with controls. Massaged premature babies: Were more alert and active Gained more weight Went home 3-6 days earlier (huge savings in costs) Most likely helps emotional bonding. Need for tactile contact when we are young. And older, too. Seniors gave each other massages. Less stress and sense of purpose. CULTURAL DIFFERENCES • • • • • • USA culture somewhat aversive to touch. Compared with South Americans and Europeans. French touch children much more than USA parents. Okay for straight men to walk hand in hand? Some cultures accept. Lots of jokes about Bush and Saudi Prince. SOMATOSENSORY SYSTEM • There are three parts • Cutaneous senses - perception of touch and pain from stimulation of the skin • Proprioception - ability to sense position of the body and limbs • Kinesthesis - ability to sense movement of body and limbs CUTANEOUS SYSTEM • Skin - heaviest organ in the body • Funtion: Protects the organism by keeping damaging agents from penetrating the body. • Layers: Epidermis is the outer layer of the skin, which is made up of dead skin cells. • Dermis is below the epidermis and contains mechanoreceptors that respond to stimuli such as pressure, stretching, and vibration. MECHANORECEPTORS • Two types located close to surface of the skin • Merkel receptor fires continuously while stimulus is present. • Responsible for sensing fine details • Meissner corpuscle fires only when a stimulus is first applied and when it is removed. • Responsible for controlling hand-grip Figure 14.1 A cross section of glabrous (without hairs or projections) skin, showing the layers of the skin and the structure, firing properties and perceptions associated with the Merkel receptor and Meissner corpuscle - two mechanoreceptors that are near the surface of the skin. MECHANORECEPTORS – GOING DEEPER • Two types located deeper in the skin • Ruffini cylinder fires continuously to stimulation • Associated with perceiving stretching of the skin • Pacinian corpuscle fires only when a stimulus is first applied and when it is removed. • Associated with sensing rapid vibrations and fine texture Figure 14.2 A cross section of glabrous skin, showing the structure, firing properties and perceptions associated with the Ruffini cylinder and the Pacinian corpuscle - two mechanoreceptors that are deeper in the skin. PATHWAYS FROM SKIN TO CORTEX • Nerve fibers travel in bundles (peripheral nerves) to the spinal cord. • Two major pathways in the spinal cord • Medial lemniscal pathway consists of large fibers that carry proprioceptive and touch information. • Spinothalamic pathway consists of smaller fibers that carry temperature and pain information. • These cross over to the opposite side of the body and synapse in the thalamus. Touch Pain The fiber carrying signals from a receptor in the finger enters the spinal cord through the dorsal root and then travels up the spinal cord in two pathways: the medial lemniscus and the spinothalamic tract. These pathways synapse in the ventrolateral nucleus of the thalamus and then send fibers to the somatosensory cortex in the parietal lobe. MAPS OF THE BODY ON THE CORTEX • Signals travel from the thalamus to the somatosensory receiving area (S1) and the secondary receiving area (S2) in the parietal lobe. • Body map (homunculus) on the cortex in S1 and S2 shows more cortical space allocated to parts of the body that are responsible for detail. • Plasticity in neural functioning leads to multiple homunculi and changes in how cortical cells are allocated to body parts. (a) The sensory homunculus on the somatosensory cortex. Parts of the body with the highest tactile acuity are represented by larger areas on the cortex. (b) The somatosensory cortex in the parietal lobe. SENSORY HOMUNCULUS SENSORY RECEPTORS FOR MOVEMENT Also on the sensory strip: Body awareness KW 10-23 VESTIBULAR SYSTEM: BALANCE Also important for body sense The labyrinth of the inner ear. It contains the semicircular canals (brown), which detect acceleration in all directions; and the otolithic organs (in the blue/purple pouches), which head orientation. Output interacts with eye movements. MOTION SICKNESS • A condition in which a disagreement exists between visually perceived movement and the vestibular system's sense of movement. • Motion is sensed by the vestibular system and hence the motion is felt, but no motion or little motion is detected by the visual system. • Car (as passenger), planes and ships. Also films. • Brain mechanism to reject poisons (nausea-vomit). • Treatment to reduce nausea: dramamine, ginger PERCEIVING DETAILS • Measuring tactile acuity • Two-point threshold - minimum separation needed between two points to perceive them as two units • Grating acuity - placing a grooved stimulus on the skin and asking the participant to indicate the orientation of the grating • Raised pattern identification - using such patterns to determine the smallest size that can be identified Methods for determining tactile acuity (a) two-point threshold; (b) grating acuity. RECEPTOR MECHANISMS FOR TACTILE ACUITY • There is a high density of Merkel receptors in the fingertips. • Merkel receptors are densely packed on the fingertips - similar to cones in the fovea. • Both two-point thresholds and grating acuity studies show these results. CORTICAL MECHANISMS FOR TACTILE ACUITY • Body areas with high acuity have larger areas of cortical tissue devoted to them. • This parallels the “magnification factor” seen in the visual cortex for the cones in the fovea. • Areas with higher acuity also have smaller receptive fields on the skin. Two-point thresholds for males. Touch most sensitive at periphery. Two-point thresholds for females follow the same pattern. PERCEIVING VIBRATION • Pacinian corpuscle (PC) is primarily responsible for sensing vibration. • Nerve fibers associated with PCs respond best to high rates of vibration. • The structure of the PC is responsible for the response to vibration - fibers without the PC only respond to continuous pressure. (a) When a vibrating pressure stimulus is applied to the Pacinian corpuscle, it transmits these pressure vibrations to the nerve fiber. (b) When a continuous pressure stimulus is applied to the Pacinian corpuscle, it does not transmit the continuous pressure to the fiber. PERCEIVING TEXTURE 1 • Katz (1925) proposed that perception of texture depends on two cues • Spatial cues are determined by the size, shape, and distribution of surface elements. • Temporal cues are determined by the rate of vibration as skin is moved across finely textured surfaces. • Two receptors may be responsible for this process - called the duplex theory of texture perception PERCEIVING TEXTURE 2 • Past research showed support for the role of spatial cues. • Recent research by Hollins and Reisner shows support for the role of temporal cues. • In order to detect differences between fine textures, participants needed to move their fingers across the surface. (a) Participants in Hollins and Reisner’s (2000) experiment perceived the roughness of two fine surfaces to be essentially the same when felt with stationary fingers, but (b) could perceive the difference between the two surfaces when they were allowed to move their fingers. PERCEIVING OBJECTS 1 • Humans use active rather than passive touch to interact with the environment. • Haptic perception is the active exploration of 3-D objects with the hand. • It uses three distinct systems • Sensory system • Motor system • Cognitive system PERCEIVING OBJECTS 2 • Psychophysical research shows that people can identify objects haptically in one to two seconds. • Klatzky et al. have shown that people use exploratory procedures (EPs) • Lateral motion • Contour following • Pressure • Enclosure Some of the exploratory procedures (EPs) observed by Lederman and Klatzky as participants identified objects. PAIN PERCEPTION • Pain is a multimodal phenomenon containing a sensory component and an affective or emotional component. • Three types of pain • 1) Nociceptive - signals impending damage to the skin • Types of nociceptors respond to heat, chemicals, severe pressure, and cold. • Threshold of eliciting receptor response must be balanced to warn of damage, but not be affected by normal activity. • More pain receptors in center of body TYPES OF PAIN • 2) Inflammatory pain - caused by damage to tissues and joints or by tumor cells • 3) Neuropathic pain - caused by damage to the central nervous system, such as • Brain damage caused by stroke • Repetitive movements which cause conditions like carpal tunnel syndrome Nociceptive pain is created by activation of nociceptors in the skin that respond to different types of stimulation. Signals from the nociceptors are transmitted to the spinal cord and then from the dorsal root of the spinal cord in pathways that lead to the brain. DIRECT PATHWAY MODEL OF PAIN PERCEPTION • Early model that stated nociceptors are stimulated and send signals to the brain • Problems with this model • Pain can be affected by a person’s mental state. • Pain can occur when there is no stimulation of the skin. • Pain can be affected by a person’s attention. COGNITIVE AND EXPERIENTIAL ASPECTS OF PAIN • Expectation - when surgical patients are told what to expect, they request less pain medication and leave the hospital earlier • Placebos can also be effective in reducing pain. • Shifting attention - virtual reality technology has been used to keep patients’ attention on other stimuli than the pain-inducing stimulation EMOTIONAL DISTRACTION • Content of emotional distraction - participants could keep their hands in cold water longer when pictures they were shown were positive The results of deWied and Verbaten’s (2001) experiment showing that participants kept their hands in cold water longer when looking at positive pictures than when looking at neutral or negative pictures. BRAIN STRUCTURES AND PAIN • Subcortical areas including the hypothalamus, limbic system, and the thalamus. • Cortical areas including S1 and S2 in the somatosensory cortex, the insula, and the anterior cingulate and prefrontal cortices. • These cortical areas taken together are called the pain matrix. Figure 14.26 The perception of pain is accompanied by activation of a number of different areas of the brain. All of these areas, taken together, are called the pain matrix. CHEMICAL OPTION: OPIOIDS AND PAIN • Brain tissue releases neurotransmitters called endorphins. • Evidence shows that endorphins reduce pain. • Injecting naloxone (opiate antagonist) blocks the receptor sites causing more pain. • Naloxone also decreases the effectiveness of placebos. • People whose brains release more endorphins can withstand higher pain levels. Ex: women giving birth (a) Naloxone reduces the effect of heroin by occupying a receptor site normally stimulated by heroin. (b) Stimulating sites in the brain that cause the release of endorphins can reduce the pain by stimulating opiate receptor sites. (c) Naloxone decreases the pain reduction caused by endorphins, by keeping the endorphins from reaching the receptor sites. PAIN IN SOCIAL SITUATIONS • Experiment by Eisenberger et al. • Participants watched a computer game. • Then, they were asked to play with two other “players” who did not exist but were part of the program. • The “players” excluded the participant. • fMRI data showed increased activity in the anterior cingulate cortex and participants reported feeling ignored and distressed. TWO COMPONENTS OF PAIN • Where am I hurt? • How much do I care?

![Shark Electrosense: physiology and circuit model []](http://s2.studylib.net/store/data/005306781_1-34d5e86294a52e9275a69716495e2e51-300x300.png)