Accountable Care Organizations: What
They Are and How Psychiatrists Can
Thrive In The Accountable Care Era
North Carolina Council of Community Programs
Medical Forum
Pinehurst, North Carolina
December 12, 2013
Julian D. “Bo” Bobbitt, Jr., J.D.
©2013 Smith Anderson
INTRODUCTION
• Part One: Elements for a successful ACO and
implementation steps which transcend provider
resource or facility and apply equally to all ACO
stakeholders.
• Part Two:
Recommended ACO strategies for
psychiatrists.
2
Part One: The Keys to ACO Success
3
WHAT IS AN ACO?
• A provider-based organization;
• That takes responsibility for healthcare needs of a defined
population;
• With goals of improving health, improving efficiency, and
improving patient satisfaction;
• That should include primary care physicians;
• And produces shared savings or other financial measures to
align incentives.
4
HOW IS THIS DIFFERENT FROM A MEDICAL
HOME?
• The Patient-Centered Medical Home (“Medical Home”)
empowers primary care to coordinate care for patients
across the continuum of care.
• It can become the core of an ACO but lacks the financial
incentives, like shared savings, to encourage providers to
deliver the highest quality at the lowest cost. It does not
involve specialists.
5
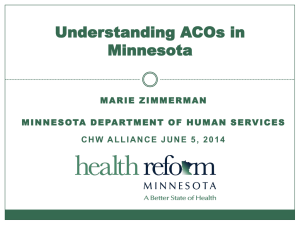
ARE ACOs REALLY COMING?
Total Spending for Health Care Under CBO’s
Extended-Baseline Scenario
• Federal taxes
and other revenues
consume about 19%
of America’s gross
domestic product
Source: Congressional Budget Office
6
RAPID TRANSITION TO REWARD VALUE
THROUGHS ACOS
• “[T]his bipartisan, bicameral discussion draft (SGR
Repeal and Medicare Physician Payment
Reform)…seeks to move away from the current
volume-based payment system to one that
rewards quality, efficiency, and innovation.”
House Ways and Means and Senate Finance Committee Staff – October 30, 2013
• Professionals with a significant portion of
revenues in risk-sharing ACOs, or related
alternative payment models, would receive a 5%
bonus each year.
7
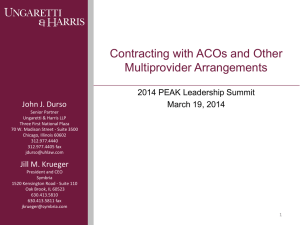
Inpatient Days Per Decedent During The Last Six Months Of Life, By Gender And Level Of Care Intensity
(Level of Care Intensity: Overall; Gender: Overall; Year: 2007; Region Level: HRR)
8
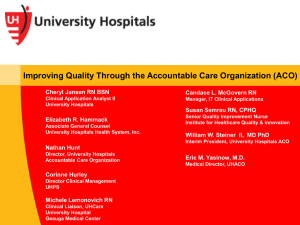
Percent Of Diabetic Medicare Enrollees Receiving Appropriate Management, by Race and Type of Screening
(Race: Overall; Type of Screening: Hemoglobin A1c Test; Year: 2003-2007; Region Level: HRR)
9
Price-Adjusted Medicare Payments per Enrollee, by Adjustment Type and Program Component
(Program Component: Overall; Adjustment Type: Price, Age, Sex & Race; Year: 2008; Region Level: HRR)
10
WHY THE U.S. HEALTH CARE SYSTEM NEEDS ACCONTABLE
CARE ORGANIZATIONS
11
THE 8 ESSENTIAL ELEMENTS OF A SUCCESSFUL
ACO
• The keys to recognizing whether to join or build an
ACO that is likely to succeed:
12
ESSENTIAL ELEMENT 1:
CULTURE OF TEAMWORK
•
•
•
•
•
•
Will be biggest challenge
Depends on Champions
Physician hurdles
Hospital hurdles
Strategic tips
Isn’t hospital employment the obvious answer?
13
ESSENTIAL ELEMENT 2:
CENTRAL ROLE OF PRIMARY CARE
•
•
•
•
Developing consensus
Recent Medical Home successes
Drivers of so many high-impact ACO initiatives
But short supply
14
ESSENTIAL ELEMENT 3: ADEQUATE
ADMINISTRATIVE CAPABILITIES
• What type of legal structure?
Network Model
(IPA, PHO,
Medical Home
Network, etc.)
Integrated Model
Payor
Payor
H
ACO
(Corp or LLC)
PCP
(Integrated Health
System – usually
through subsidiary or
affiliate entity)
PCP
Contract
SPEC
Contracts
PCP
S
PCP
S
H
Optional
Contracts
PCP
15
ESSENTIAL ELEMENT 3: ADEQUATE ADMINISTRATIVE
CAPABILITIES (cont’d.)
• Functional Capability 1 – Performance Measurement
• Functional Capability 2 – Financial Administration
• Functional Capability 3 – Clinical
16
ESSENTIAL ELEMENT 3: ADEQUATE
ADMINISTRATIVE CAPABILITIES (cont’d.)
• Who should be in an ACO?
– All primary care?
– What about specialists?
– What about hospitals?
– What about community partners?
• How many in a region?
17
ESSENTIAL ELEMENT 4: SUFFICIENT FINANCIAL INCENTIVES TO
PROMOTE SHARED ACCOUNTABILITY
• Three tiers of ACO financial
incentives
– “Asymmetrical” – Shared
Savings
Symmetrical – Savings
Bonus and Penalty
Capitation
Savings Based on Spending Targets
Fee For
Service
Low Risk
Shared
Savings
Shared
Savings +
Penalty
Capitation
High Risk
18
ESSENTIAL ELEMENT 5: HEALTH INFORMATION
EXCHANGE CAPABILITY AND DATA
• What data?
– Baseline – for comparison
– Performance metrics – aligned with initiatives
– Clinical support – at the point of care
• Who gathers it?
• Who decides?
19
ESSENTIAL ELEMENT 5: HEALTH INFORMATION
EXCHANGE CAPABILITY AND DATA (cont’d.)
Basic EHR
HIE
ACO IT Infrastructure
• Data mining capabilities to
contribute to financial impact
modeling, value reporting, and payor
negotiations
• Decision support capabilities at point
of care
• Expanded access to patient records
across the continuum
• Comparative data collection to
determine gaps in care delivery
processes and outcomes vs. peers
Functional
Complexity
• Patient health information
available at point of care
• Reporting capabilities to state
and federal agencies
• Patient health information
available at point of care
• Reporting capabilities to state and
federal agencies
• Patient health information available
at point of care
Scope of Information Sharing
20
ESSENTIAL ELEMENT 6: BEST PRACTICES ACROSS THE
CONTINUUM OF CARE
• Top targets:
–
–
–
–
–
Prevention
Chronic disease management
Reduced hospitalizations
Care transitions across fragmented system
Multi-specialty management of complex patients
• Match ACO strengths to greatest community gaps in care
needs
21
ESSENTIAL ELEMENT 7:
PATIENT ENGAGEMENT
• What can an ACO do to engage patients?
• Why is it so important?
22
ESSENTIAL ELEMENT 8: SCALE-SUFFICIENT PATIENT
POPULATION
• Economies of scale; savings pool
• How a start-up ACO can get there
23
THE 8 ESSENTIAL ELEMENTS OF A SUCCESSFUL
ACO
24
Part Two: Applying the ACO Strategies to
Psychiatrists
25
WHY CARE? – PRO
• Return of control of physician/patient relationship
• Leverage your power to heal
• With > one-half primary care physician visits
associated with psycho/social issues, averaging 2x to
3x the costs, psychiatrists well positioned for pay-forperformance
• Essential to be in “narrow network” because of
aggressive payor steerage to them
• America rapidly moving away from fee-for-service to
value-based payment
26
WHY CARE? – CON
•
•
•
•
•
No time, no war chest, no experience
Some ACOs don’t include psychiatry
Hard to be interdependent with others
This too shall pass
Being unprepared is an option
27
ACO INITIATIVES
• Review Top ACO Initiative Areas:
–
–
–
–
–
Prevention/wellness
Chronic disease management
Transitions across fragmented system
Reduced hospitalizations
Multi-specialty complex patient management
• What is the best match for your ACO’s strengths and
the market’s greatest needs/gaps in care?
• Where do psychiatrists fill those gaps?
28
PSYCHIATRY’S POTENTIAL TO ADD VALUE (AND
RECEIVE CORRESPONDING REWARD)
• Psychiatric disease as a co-morbidity “is the rule
rather than the exception” in high-cost cases. (Robert
Woods Johnson)
• The ACO approach accepts the premise that
treatment for general physical care must be
integrated with mental health and substance abuse
treatment.
• Impact Model shows benefit.
29
PSYCHIATRY’S POTENTIAL TO ADD VALUE
30
RECOMMENDED ACCOUNTABLE CARE
INITIATIVES
• The psychiatrist as leader of ACO Behavioral Health
Team
o Stepped Care
o Develop systematic pcp screening program for psychiatric
illness
o Treatment guidelines
o Onsite collaboration with pcp
• Avoid expensive drugs with marginal value
• Patient communication
• Telepsychiatry
31
WE’VE GOT SOME GREAT VALUE-ADD
CONTRIBUTIONS—NOW WHAT?
• Pick the right ACO(s)
• Have them want to pick you
o
o
o
o
Relationships
Have a compelling story
Primary care is the client
Protect your legal and financial interests
32
METRICS ARE KEY
• You must own the metrics.
• They should reflect each selected initiative’s tasks
(process) you want to occur and goals (outcomes)
you want to achieve.
• Do not waste your contributions: even if you do a
great job, if the metrics are off, you will not be
rewarded.
33
HOW DO I ASSURE THAT THE SAVINGS POOL
DISTRIBUTION IS FAIR?
34
CONCLUSION: IT’S A
GOOD PROBLEM TO HAVE!
• THANK YOU!
• QUESTIONS?
Julian D. “Bo” Bobbitt, Jr.
Smith Anderson Blount Dorsett Mitchell & Jernigan, LLP
Post Office Box 2611
Raleigh, North Carolina 27602-2611
919-821-6612
bbobbitt@smithlaw.com
35